



INTRODUCTION
The elderly in Indonesia range from the age above 55 years. The proportion of the elderly in Indonesia increased from 1.1% to 6.3% of the total population. The process of the elderly affects various aspects, such as physical, psychological, biological, and social changes. Decreased bone mass is one physical change that occurs with age.[1]
Osteoporosis decreases bone mass density and worsens bone microarchitecture, so bones become brittle and easily fractured. Fractures can occur in any bone, but the most frequent locations are the hip, spine, and wrist.[2]
The Ministry of Health of the Republic of Indonesia stated in 2012 that women have a higher risk of osteoporosis than men, which is 21.7% vs. 14.8% because women pass through several periods such as pregnancy, breastfeeding, and estrogen reduction in premenopausal, menopausal and postmenopausal.[3]
The risk of osteoporosis and bone fractures increases with age, 1 in 3 women over 50 has had a bone fracture during their lifetime. The incidence of osteoporosis fractures is relatively high, especially in the age group of 50 years, around 40% to 50% in women and 13% to 22% in men.[2,4]
Two thousand nine statistics state that 200 million people worldwide have osteoporosis, and it is estimated that by 2050 there will be 6.3 million people who experience pelvic fractures every day, increased 2-fold in females and 3-fold in males. The World Health Organization (WHO) shows that 50% of fractures are in the fractures of the upper femur, which can result in disability and death.[5,6]
The WHO fracture risk assessment tool (FRAX) calculation data in 2011 showed the highest incidence of pelvic fractures in the female sex at the age of 95 to 99 years, with as many as 1,680 cases, and the lowest in aged 40 to 44 years, there are 8 cases. The incidence of pelvic fractures in the male sex was highest at the age of 90 to 94 years, with as many as 718 cases, and the lowest at 0 to 44 cases, as many as 10 cases.[6]
The International Osteoporosis Foundation notes that about 20% of osteoporotic patients who experience fractures die within a year. One-third of them need to be in bed, and another third need help standing and walking. Only the remaining third can heal and perform optimally.[7]
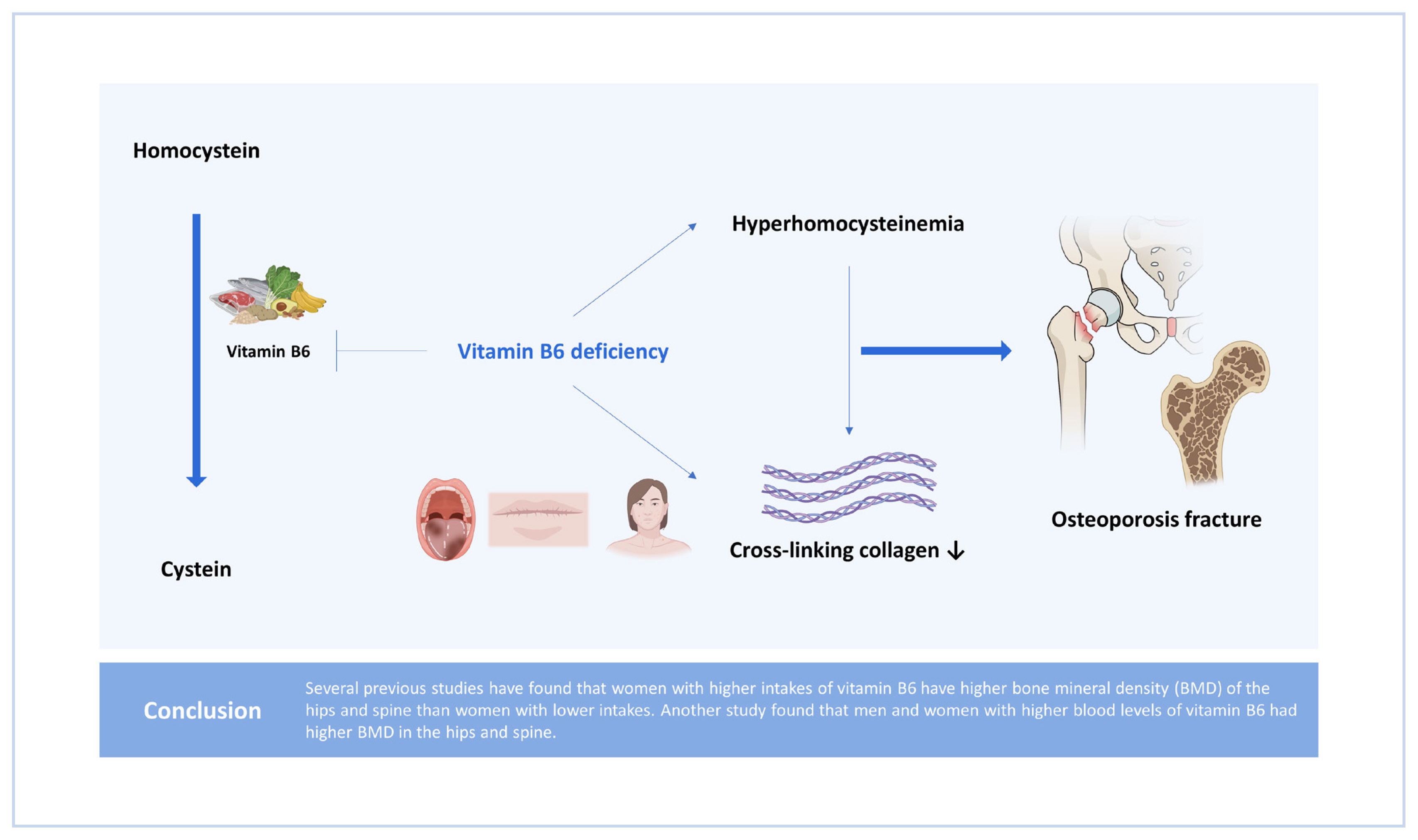
Many factors cause the occurrence of osteoporotic fractures; one of these factors is hyperhomocysteinemia. Hyperhomocysteinemia hurts bones that cause impaired collagen formation cross-linking, which causes bones to become brittle and fracture easily. Homocysteine is a form of methionine demethylation, potentially at risk of osteoporosis fractures. High plasma homocysteine levels are associated with bone loss velocity.[2,8]
ROLE OF VITAMIN B6
Vitamin B6 is a cofactor of more than 100 enzymes that catalyze metabolic reactions, especially amino acid metabolism, in transamination, decarboxylation, or aldolase activity. Vitamin B6 also plays a role in carbohydrate metabolism (as a coenzyme glycogen phosphorylase) and lipid metabolism in the biosynthesis of sphingolipids and carnitine.[2,10]
B vitamins play a role in the process of growth, development, and functions in the body by regulating the activity of enzymes. Vitamin B6 specifically plays a role in synthesizing neurotransmitters, epinephrine, and hemoglobin synthesis, as well as a physiological mediator for the function of steroid hormones, namely as a negative control of the work steroid hormones.[11,12]
STABILITY AND BIOAVAILABILITY OF VITAMIN B6
Vitamin B6 in foodstuffs is stable in acidic conditions and unstable in neutral and alkaline (alkaline) state exposed to heat and rays (light). The cooking and heating process lowers vitamin B6 levels (up to 70%), while storage and preservation lower B6 levels more slowly. PN heating is much more stable than PL and PM.[2,11]
ABSORPTION, METABOLISM, AND EXCRETION OF VITAMIN B6
Vitamin B6 is absorbed in non-phosphorylated form mainly in the jejunum and ileum using passive diffusion, but the hydrolysis of certain phosphate ester compounds occurs during the digestive process. Once absorbed, PN, PL, and PM are released in circulation from the port and then taken by the liver. In the liver, the vitamer is almost converted into the state of PLP, so PLP is the main vitamer form found in the systemic circulation and the main metabolically active form of vitamin B6.[2,10]
As much as 50% of the amount of vitamin B6 in the body is stored in the muscles. PLP in the liver is bound by apoenzymes and circulates in the blood bound to albumin. The metabolic results of vitamin B6 are mainly excreted through urine in the form of 4-pyridoxic acid (4-PA). About 40% to 60% of vitamin B6 consumed is estimated to be converted into 4-PA.[13,14]
VITAMIN B6 STATUS ASSESSMENT
The status of vitamin B6 can be determined directly and indirectly. It can be done now by measuring the concentration of PN in plasma, red blood cells, and urine. Indirectly, by measuring erythrocyte aminotransferase activity, excretion of tryptophan metabolites, and measurement of the concentration of 4-PA in the urine.[11]
VITAMIN B6 ADEQUACY
The recommended adequacy of vitamin B6 in Indonesia is for the age group of 30 to 49 years, men equal to women at 1.3 mg/day, at the age of ≥50 years, for men 1.7 mg/day, while for women 1.5 mg/day.
FOOD INGREDIENTS SOURCE VITAMIN B6
Sources of vitamin B6 are widely distributed in animal and vegetable source foodstuffs. PN is the main vitamer in plant foodstuffs, while PL and PM are mainly found in animal foodstuffs. Foods high in vitamin B6 include liver, meat, mackerel, fish, avocado, bananas, eggs, beans, poultry, potatoes, and whole-grain products, especially flour, vegetables, beans, and fortified cereals.[2,10]
VITAMIN B6 DEFICIENCY
Vitamin B6 deficiency can occur in any fault part of a thorough vitamin B deficiency complex. Vitamin B6 is widespread in the diet, so it is rare for defects to occur due to a lack of daily intake. The populations at risk of vitamin B6 deficiency are elderly, pregnant, breastfeeding, excessive consumption of alcohol, impaired liver and kidney function, as well as the consumption of certain medications such as isoniazid, cyclocystine, penicillin, and hydrocortisone.[2,10]
Vitamin B6 antagonists derived from foodstuffs such as agrarian, gyrotron (fungal variations), and Latin (flaxseed group) can inhibit vitamin B6 metabolism. Neuroflavin, niacin, and zinc deficiency can also cause vitamin B6 deficiency because these 3 nutrients are needed as cofactors for the interconversion and metabolism of vitamin B6. Symptoms of vitamin B6 deficiency are not typical of fatigue, drowsiness, headache, peripheral neuropathy, oral lesions (glossitis, cheilosis, stomatitis), impaired immunity, convulsions, depression, and microcytic hypochromic anemia. Skin and nerve disorders are the most widely reported clinical manifestations.[11]
OSTEOPOROSIS
Osteoporosis is a systemic bone disease characterized by a decrease in bone mass density and a worsening of bone microarchitecture so that bones become brittle and easily fractured. Osteoporosis is defined as a condition in which bone mineral density (BMD) is below the reference value according to age or standard deviation.[2,5]
SYMPTOMS OF OSTEOPOROSIS
Osteoporosis is a progressive disease that occurs for many years without symptoms. Complaints with osteoporosis may arise only in pain and discomfort in the back or bone area. Fractures can occur only due to minimal shaking or impact on the bones that withstand the body’s weight. The pain can go away in a few days or weeks, but it arises if osteoporosis occurs again in other places.[13]
Symptoms at an advanced stage include fractures, an increasingly bent back, reduced height, or back pain. Decreased bone density will cause bones to be easily destroyed, and bone pain and bone deformity will arise. Spinal ruins cause chronic back pain.[5]
RISK FACTORS
Risk factors for osteoporosis include age, gender, low body mass index, previous fracture history, family history with pelvic r-fracture, smoking, consumption of alcohol (≥3 cups per day), and glucocorticoid treatment (>5 mg of prednisolone per day for ≥3 months).[2]
Division of risk factors for osteoporosis:
-
1. Mutable factors
-
2. Irreversible risk factors
• Family history
• Gender: Female
• Age
• Asian and Caucasian races
• Menopause[6]
OSTEOPOROSIS FRACTURE
The best standard currently in the diagnosis of osteoporosis is the measurement of BMD in the hip using the dual energy X-ray absorptiometry method. The fracture diagnosis is established based on the clinical evaluation of osteoporosis linked to the fracture site. The WHO recommends a FRAX related to BMD measurements for the identification of high-risk individuals.[2,14]
IMPACT OF OSTEOPOROSIS FRACTURE
The location of the fractured bone distinguishes types of osteoporotic fractures. The most frequent sites are the pelvis, spine, and wrists. Pelvic fracture is the most severe osteoporotic fracture with a reasonably high morbidity and mortality rate. Spinal fractures are usually diagnosed after a 21% decrease in spinal height. Wrist fractures increase after women enter menopause and are constant after age 65.[2]
The impact of an osteoporosis fracture is an increase in the socioeconomic burden in the form of enormous treatment costs. Osteoporosis fractures can result in disability and dependence on others, which can impair life activities, social functions, and psychological disorders so that there is a decrease in the quality of life, even to the point of causing death.[7]
PATHOPHYSIOLOGY
Cross-linking collagen is one of the parts that play an essential role in maintaining bone strength. Cross-linking collagen determines the strain quality and viscoelasticity of the bones, and an abnormal state will lead to bone fragility or harness. Impaired enzymatic cross-linking processes and hyperhomocysteinemia will cause poor-quality bone collagen.[2]
EFFECT OF VITAMIN B6 ON HOMOCYSTEINE METABOLISM
Homocysteine is part of the amino acids formed during methionine metabolism. Methionine sources include meat, fish, vegetables, fruits, nuts, and whole grains. Methionine is the only known source of homocysteine. Homocysteine metabolism passes through 2 pathways: transsulfuration and remethylation. The transsulfuration pathway occurs when cysteine synthesis is required, so homocysteine enters into this pathway. This reaction requires the enzyme cystathionine-β synthase and vitamin B6 as cofactors.[15]
Hyperhomocysteinemia is thought to be a new factor in the risk of osteoporosis fractures. Epidemiologically and clinical trials show hyperhomocysteinemia increases the risk of fractures. Vitamin B6 has 2 roles in homocysteine metabolism: remethylation and transsulfuration pathways, the most critical role crucial transsulfuration pathways.[2,12]
Plasma concentrations of homocysteine are determined by the metabolism associated with B vitamins, one of them vitamin B6. The average homocysteine concentration in plasma is 5 to 15 μmol/L.[15,16]
Hyperhomocysteinemia affects bone extracellular matrices caused by the breakdown of cross-linking collagen. It is reported that vitamin B deficiency is associated with a decrease in cross-linking enzymes in human bones. Therefore, hyperhomocysteinemia and vitamin B6 deficiency affect bone quality and disturbances in cross-linking collagen.
The PLP form plays a vital role in the homocysteine transsulfuration reaction as a cofactor of the enzymes stationing β-synthase and cystathionine γ-lyase that converts homocysteine into cysteine. In the remethylation pathway, vitamin B6 also plays an indirect role as a cofactor of the serine hydroxymethyl transferase and glycine decarboxylase enzymes. Both enzymes play a role in helping folate as a methyl donor in the reaction of remethylation of homocysteine into methionine.
Research by Herrmann et al. [12] and Koh et al. [17] showed increased homocysteine concentrations, thereby increasing osteoblast activity and bone biopsies. Other studies have also demonstrated indications that high concentrations of homocysteine inhibit the activity of lysyl oxidase (LOX; an enzyme involved in cross-linking collagen) and stimulate osteoclasts. Disturbances in cross-linking collagen will cause bone matrix changes, making bones brittle.
Van Wijngaarden et al. [18] research in 12 elderly patients showed a significant association between increased fracture risk. It increased total homocysteine concentration during follow-up between 3 and 12 months. Furthermore, the research of Dai et al. [19] on 63,154 Chinese men and women aged 45 to 74 years showed a relationship between vitamin B6 and the risk of pelvic bone fractures only in women.
The research of Yazdanpanah et al. [20] on 5,305 Dutch men and women aged 55 years by evaluating the administration of some vitamins B showed a positive relationship between the administration of vitamins B6 with mass bone density, where there is a 23% decrease in the risk of fractures. Meanwhile, McLean et al. [21] conducted a study on 1,002 white men and women in the US aged 75, showing a relationship between vitamin B6 and the risk of bone fractures pelvis, and those risks are associated with homocysteine (Table 1).
A decrease in plasma concentrations of homocysteine was seen after the administration of vitamins B, one of them by vitamin B6 in the study of Green et al. [22] on 276 healthy older adults over the age of 65 years for 2 years, while the low serum folate and vitamin B6 are associated with changes in bone morphology which is an analysis of the study of Holstein et al. [23] of 94 men and women (Table 1).
EFFECT OF VITAMIN B6 ON CROSS-LINKING COLLAGEN
Osteoporosis is a disease caused by disorders of the bone matrix. The collagen matrix plays a vital role in the normal bone formation process and requires cystitis of cross-linking collagen. Homocysteine interferes with the formation of cross-linking collagen, which is part of the normal bone collagen synthesis process. Patients with hyperhomocysteinemia can aggravate the occurrence of osteoporosis.[15]
Collagen is a strong interrelated structure analogous to a bridge (cross-linking). This function of collagen allows the occurrence of elasticity and bones that have flexibility and strength. It helps to assess bone quality from the collagen side.[24]
The enzymatic formation of cross-linking is controlled by 2 enzymes, namely lysine hydroxylase and LOX, with PLP being a coenzyme. LOX is an enzyme secreted by osteoblasts. Vitamin B6 deficiency exhibits an effect on cross-linking formations. Some studies show bone LOX activity drops with age. In addition, plasma PLP levels drop by about 0.9 ng/mL per decade, so in the elderly, especially those with low vitamin B6 status, bones can become brittle and easily fracture.[2,25]
Vitamin B6 works as an essential enzyme required by cross-linking collagen; low levels of vitamin B6 can affect cross-linking collagen and cause bone quality to be impaired. In addition to its role in LOX, vitamin B6 works as a substrate of alkaline phosphatase in bone formation and regulates the balance of osteoblasts and osteoclasts.[16,26]
Dietary modifications can lower an increase in homocysteine concentration. The US Department of Agriculture recommends consuming 2 to 4 servings of fruit, 3 to 5 servings of vegetables, and 6 to 11 servings of bread, grains, and pasta.[15]
EFFECT OF VITAMIN B6 ON OSTEOPOROSIS FRACTURES
The role of vitamin B6 in osteoporotic fractures is estimated to be through homocysteine metabolism, and some homocysteine plays a role as a regulator of cross-linking collagen formation. Hyperhomocysteinemia and low B vitamins directly affect bone metabolism by stimulating osteoclast activity while reducing osteoblast activity.[27]
CONCLUSION
Osteoporosis fracture is an advanced infection of osteoporosis that provides clinical complaints and symptoms. Collagen is the most significant component of the bone matrix, so interference with the formation of cross-linking collagen will increase the risk of fractures. Vitamin B6 acts as a regulator of cross-linking collagen formation. Vitamin B6 deficiency is associated with decreased bone strength through the mechanism of disruption in collagen cross-linking both directly and in homocysteine-related pathways.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






