



INTRODUCTION
In patients with prostate cancer, bone is a dominant site of metastasis.[1] Bone metastases often lead to bone mineral density (BMD) decreases, bone fractures, spinal cord compression, and pain. In addition to bone metastases, other primary contributors to bone fragility in prostate cancer patients include aging-related bone loss as well as androgen-deprivation therapy (ADT), which increases the risk of osteopenia, osteoporosis, and fractures.[2,3] Osteoporosis is present in up to 42% of prostate cancer patients even before they start ADT.[4] Prostate cancer patients receiving ADT have been reported to experience BMD losses in the lumbar spine, total hip, and femoral neck, contributing to the diagnosis of osteoporosis.[4] Bone loss and osteoporosis greatly increase the risk of sustaining debilitating fractures; thus, fracture prevention is a major concern in prostate cancer patients.[5]
BMD derived from dual energy X-ray absorptiometry (DXA), often combined with a fracture risk assessment tool (FRAX) score, is the standard of care for determining fracture risk. While BMD and BMD T-score are used to determine bone strength, the role of FRAX in determining fracture risk in patients with cancer-associated bone disease has not been standardized.[6] FRAX does not account for the effect of malignancy and treatment on fracture risk. There is a need for additional diagnostic measures to assess for fracture risk in prostate cancer patients.
The 18F sodium fluoride (18F-NaF) is an U.S. Food and Drug Administration-approved radiotracer for monitoring metastatic bone disease using positron emission tomography/computed tomography (PET/CT).[7-9] 18F-NaF PET/CT is currently used to evaluate both disease progression in the bone and response to prostate cancer treatment [10,11]; simultaneously, it functions as a powerful tool to study bone formation and healing from fracture.[12-14] Recently, 18F-NaF PET/CT has been shown to be useful in detecting age-related changes in bone metabolism.[15,16] Since fracture strength of metastatic bone depends on the lesion location,[17] the ability to assess localized bone metabolism could provide information not captured by global imaging markers. However, the application of 18F-NaF PET/CT markers in assessing fracture risk in prostate cancer patients is not well established. Therefore, it would be useful to investigate the potential for opportunistic osteoporosis assessment and fracture risk reduction with PET/CT.[15,18-21]
The purpose of this study was to assess whether bone deposition, assessed by 18F-NaF uptake in 18F-NaF PET/CT scans, could predict incident fractures better than DXA- or CT-derived BMD in prostate cancer patients.
METHODS
1. Data collection
This retrospective study utilized clinical data from patients of our institution’s healthcare system. The study protocol was approved by the Institutional Review Board and exempted from continuing review. Written consent was not obtained from patients as all data was de-identified.
The study included patients with a history of prostate cancer who had undergone 18F-NaF PET/CT imaging. The 112 male patients were identified as having full-body 18F-NaF PET/CT scans available for image analysis. Criteria for inclusion were male sex, availability of 18F-NaF, and diagnosis of prostate cancer. Criteria for exclusion were extensive spinal metastases (4 patients), SUVmean and SUVmax values less than 2 standard deviations from the mean (1 patient), or corrupted PET/CT images (2 patients). Of the initial 112 patients with imaging, 105 patients (ages, 53-91 years; mean age, 70.8; mean body mass index [BMI], 29.2 kg/m2) met these criteria and were retained in the study.
The data sampling time was from January 2012 to December 2019. Demographic, cancer therapy and fracture information were obtained from electronic medical records, whereas 18F-NaF PET/CT and DXA data were obtained from radiological records.
Each patient chart was searched thoroughly for the incidence of clinical fractures subsequent to the scan. The keywords “fracture”, “fx”, “frax”, “osteoporotic fracture”, “break”, and “compression” were used. All body fractures were recorded and subsequently categorized by location: spine, ribs, hip, arm, leg, and foot bones. The time of fracture(s) relative to PET/CT date was recorded.
2. Imaging acquisition
18F-NaF PET/CT images were obtained 66.0 (60.0-74.7) min after intravenous injection of 8.6 (5.4-10.5) mCi 18F-NaF, both reported as median (interquartile range).
3. Image analysis
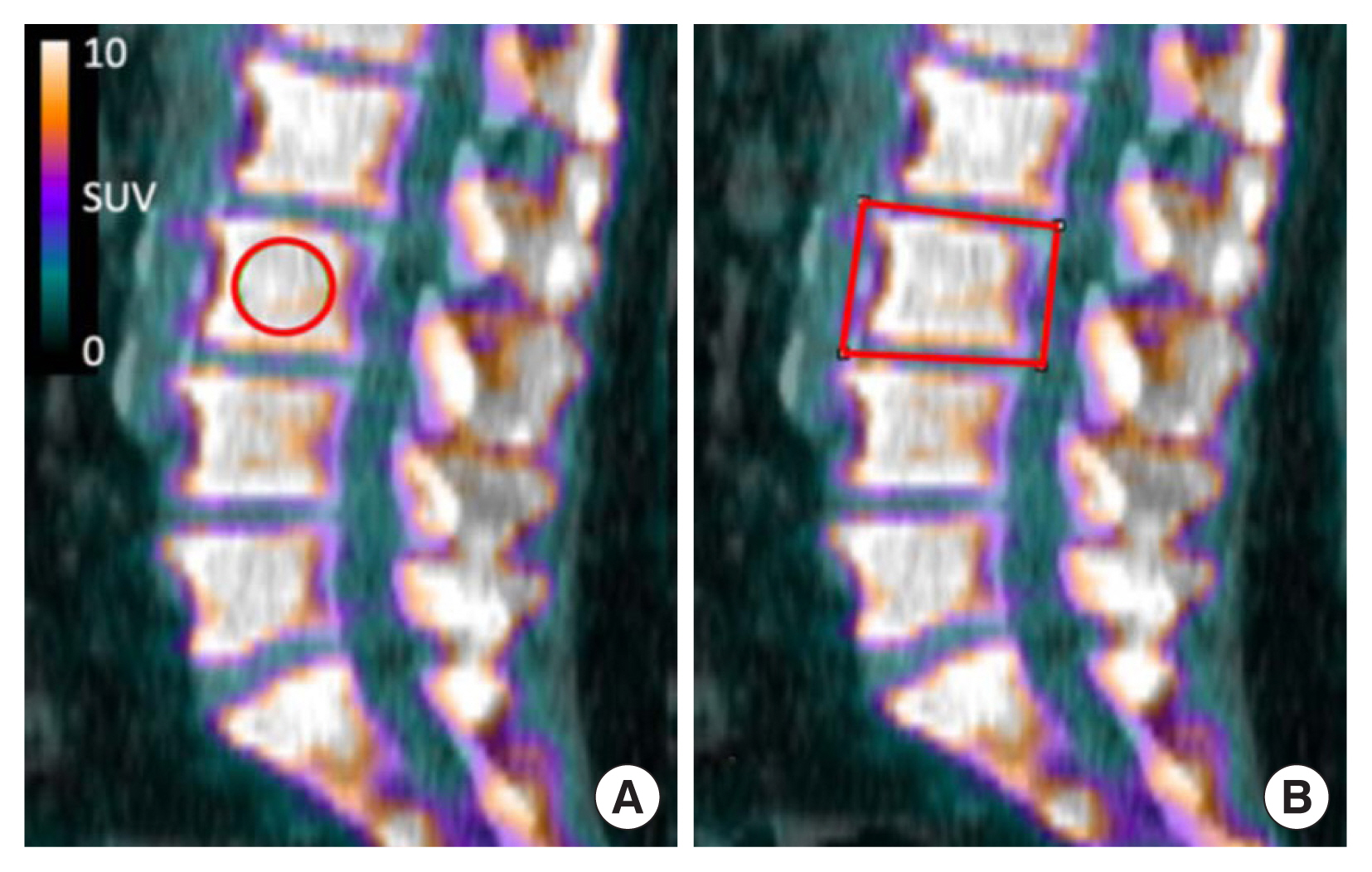
A PET/CT image processor (Fiji PET/CT Viewer Plug-in, Beth Israel) was used to measure 18F-NaF standardized uptake values (SUVmean and SUVmax) of each vertebra from C2 to S1 in a single-slice rectangular region of interest (ROI) outlining the vertebral body at the midline sagittal view. The midline was determined by selecting the slice where the spinous processes were at their largest in the sagittal view. As a quality control measure, SUVmean and SUVmax were also measured in a spherical ROI at the center of the vertebra, with a 10 mm diameter for all vertebrae except for T12-L5, where a 20 mm diameter was more suited to the larger volume (Fig. 1). Within the rectangular ROI, SUVpeak (the SUVmean in a 1 cc volume centered on SUVmax) and SUVqpeak (the average of SUVmax together with the 3 hottest pixels in a 1 cc volume, centered on SUVmax) were obtained to reduce the statistical fluctuation of a single pixel SUVmax. CT-derived Hounsfield units (HUs) were also obtained via the rectangular ROI. Throughout the paper, R and S will be used to reference measures obtained with a rectangular and spherical ROI, respectively.
Care was taken to avoid areas of metastases as identified using radiologist reports. In cases where metastases could not be avoided, the vertebra was omitted from the analysis. A total of 34 vertebras were omitted across all patients. Several omissions came from the same patient in cases with extensive but avoidable metastases in the spine.
Average cervical, thoracic, lumbar, sacral, and spinal SUVmean, SUVmax, SUVpeak, SUVqpeak, and HU were calculated for each participant. The first cervical vertebra and lower sacral vertebrae (S2 and below) were not differentiable on the scans, therefore C2-C7 and S1 values were used to assess cervical and sacral spines, respectively.
4. Statistical analysis
T-tests were used to determine the difference in cervical, thoracic, lumbar, sacral, and average 18F-NaF uptake (SUVmean, SUVmax, SUVpeak, and SUVqpeak) between 2 groups: a group which developed an incident fracture (after their scan) anywhere in the body, and another group which did not. CT-derived HU measures have previously been shown to correlate with clinical standard DXA BMD.[22-25] Average baseline HU measurements were also compared between the fracture vs. no-fracture groups.
Participants were also divided by the incidence or non-incidence of compression fractures in the spine, as opposed to fractures anywhere in the body. HU values were compared with t-tests between these 2 groups.
Age, BMI, time to scan and tracer dose were also compared between the 2 groups, looking at all fractures or compression fractures. For patients who underwent DXA, baseline BMD, BMD T-Score, average SUVmean and SUVmax were compared amongst groups with and without fractures using t-tests.
RESULTS
1. Cohort characteristics and fracture data
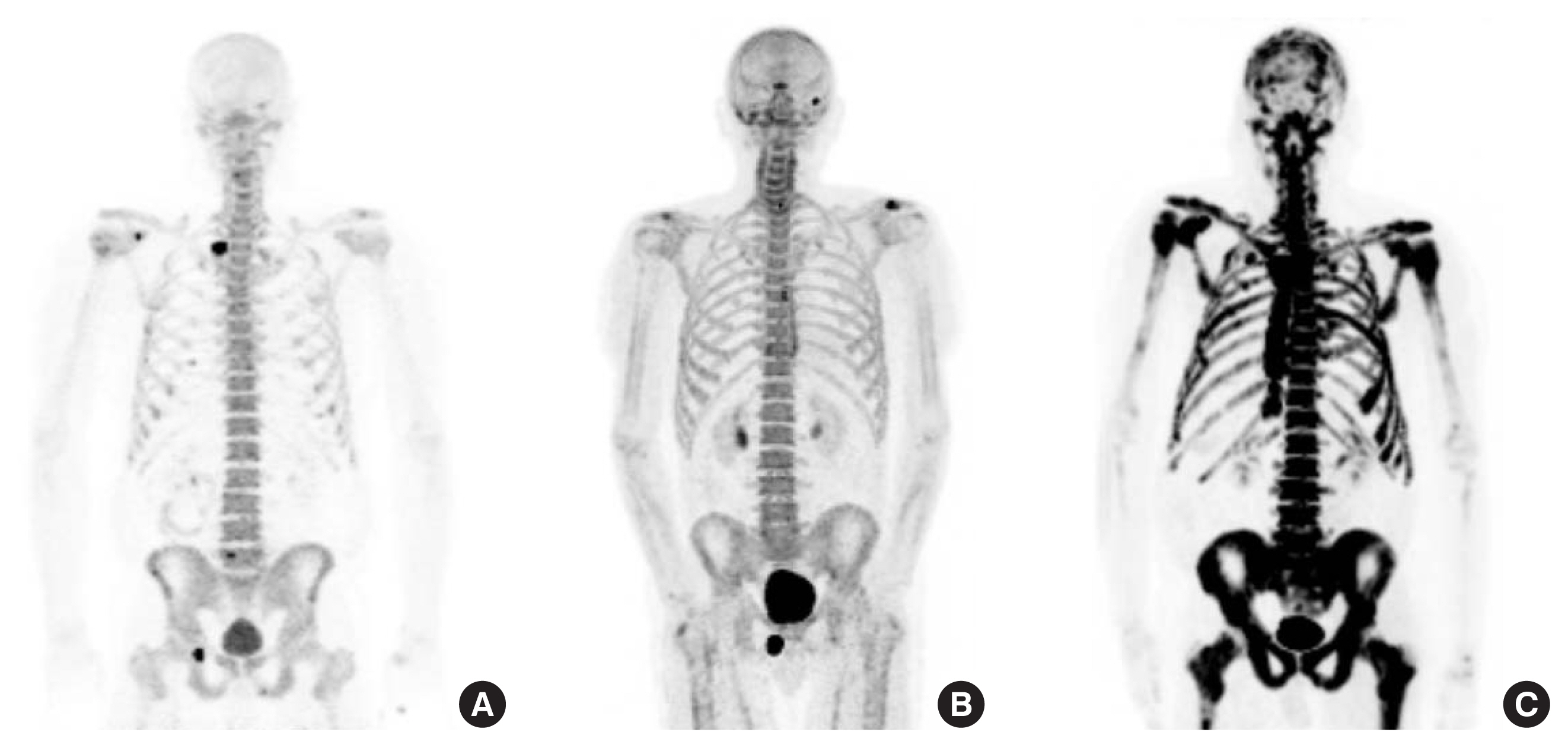
Of the initial 112 patients with full body scans, 4 patients were excluded from the analysis due to extensive metastases in the spine that could not be avoided during segmentation, and 1 patient was excluded due to exceptionally low uptake (spine SUVmean, SUVmax, SUVpeak and SUVqpeak measures less than 2 standard deviations from the rest of the cohort) (Fig. 2). Two patients had scans that could not be opened by the imaging software. The total number of patients included in the study was therefore 105. Patient illness and treatment information is detailed in Table 1.
Twenty-seven out of the 105 patients reported at least one bone fracture after the 18F-NaF PET/CT scan (Table 2). Some patients had multiple incident fractures. The major fractures were compression fractures of the spine (N=14), rib fractures (N=8), hip/femur fractures (N=6), and long bones (N=6). The mean (standard deviation) time between the PET/CT scan and the fracture was 3.1 years (2.5).
2. Deposition and HU
Thoracic SUVmean (in rectangular ROI, R, and spherical ROI, S), SUVmax (R, S), SUVpeak (R), and SUVqpeak (R) were all lower in the group with incident fractures (at least one fracture, anywhere in the body) than in the no-fracture group (P<0.05 for all). Thoracic HU (R) was not different between the 2 groups (P=0.3708). After accounting for differences in administered tracer dose, 18F-NaF uptake in the thoracic spine remained significantly lower in the fracture group (Table 3), in all measures except for thoracic SUVmax (S). Age, BMI, time to scan were not different between the 2 groups. Cervical, lumbar, and sacral 18F-NaF uptake and HU were also not different between the 2 groups.
When combining all vertebras, there was a significant difference in total spine SUVmean (R, S), SUVmax (R, S), SUVpeak (R), and SUVqpeak (R), (P<0.05 for all) with no difference in spine HU (P=0.087). This difference in spine SUV disappeared when correcting for dose.
An analysis considering only future compression fractures (14 patients) yielded similar results as above. Thoracic and whole spine 18F-NaF were again lower in the compression group but the significance disappeared after correction for dose. One difference was that HU of the spine was lower in patients who developed incident compression fractures (Table 4). Lower HU was observed in the cervical and sacral spine of patients with future compression fractures but not in the thoracic and lumbar regions.
3. DXA
Of the 105 patients in the final cohort, 40 also had DXA scans on file. Of those, 13 patients with DXA scans had fractures. DXA characteristics are described in Table 5. Lumbar BMD, BMD T-score, and BMD Z-score were not correlated with the incidence of fractures or compression fractures.
DISCUSSION
Our retrospective study reports an appreciably lower thoracic vertebral bone deposition as measured by 18F-NaF uptake in prostate cancer patients with incident bodily fractures. The lower thoracic bone deposition was associated with fractures but not lower thoracic bone density, suggesting the thoracic spine as a potential area of interest in fracture prediction in prostate cancer patients with access to an 18F-NaF PET/CT scan. Cervical, lumbar, and sacral 18F-NaF uptake, as well as age and BMI, were not significantly different in fracture versus no-fracture groups. CT-derived BMD measures were also not different between the 2 groups.
One possible explanation for our findings is that patients who undergo chemotherapy or radiotherapy experience bone loss which not only reduces bone metabolism of the spine but also increases the risk for fracture.[26,27] We observed no significant difference in CT-derived BMD between the fracture and no fracture groups to confirm this. We did see a lower CT-derived BMD in the cervical and sacral regions of 14 patients with incident compression fractures but not in the thoracic or lumbar regions. It is worth nothing that CT-derived BMD, measured in HU, is not a perfect correlate to DXA-derived BMD. Yet, in patients who received DXA scans (40 out of 105), BMD and associated markers (T-score and Z-score) were not significantly different in groups with and without incident fractures, suggesting the poor fracture-predictive ability of DXA in this population.
The possibility that a slow-down in the deposition of new bone material precedes bone loss and fractures is also a plausible explanation for the observed differences in bone deposition between the fracture and non-fracture groups despite comparable thoracic CT-derived BMD measures. Vertebral fractures are most common between T8 and L4, [28] which suggests that changes in bone deposition may occur earlier in the thoracic and lumbar spine before affecting other areas of the spine.
The potential confounder of metastasis to bone is an important consideration in interpreting the results of this study. Prostate carcinomas have a propensity to metastasize to the spine, with a decreasing involvement from the lumbar to thoracic to cervical spine hypothesized to be caused by an upward metastatic spread along spinal veins after initial lumbar metastasis. In one study, Amelot et al. [29] found that prostate cancer was associated with L1-L4 and T8 metastases. It has also been noted that pelvic and spinal metastases are most common in patients with fewer lesions, suggesting that such lesions occur early in the disease progression.[30] Bony metastases can increase the uptake of 18F-NaF. Given the involvement of the lumbar spine in the metastatic progression of the disease, an increase in lumbar 18F-NaF uptake is expected to correlate with a poorer oncologic prognosis and an increased risk for fractures. This study omitted from analysis all vertebrae with metastases, yet metastatic involvement of the spine could have been missed or invisible on the scans. Undetected metastases could potentially raise 18F-NaF uptake in the spine, particularly in the lumbar spine, where metastasis is more likely. In addition, such an overestimation would likely be more pronounced in the fracture group due to the demonstrated association between metastasis and fracture. However, the authors of this study consider this effect unlikely because it would not be expected to spare the thoracic spine, where lower uptake in the fracture group was clearly observed.
Our study has some limitations. We controlled for multiple variables that may influence SUV, such as age, BMI, tracer dose, and uptake period; however, we did not extend this to include other variables of interest, including patient factors such as mobility, blood sugar, or therapy duration, and scanner differences on SUV. While we did not analyze the effect of each therapy on fracture incidence, it is of note that our cohort is sufficiently therapeutically diverse to be representative of the prostate cancer patient population. Other limitations to our study include the retrospective collection of data entailing limited availability of data points near in time to the scan. BMI was especially affected with some time points at a maximum 2 months before or after the scan. Retrospective data collection also limits our characterization of fractures as pathologic, traumatic, or insufficiency fractures, and we did not assess whether fractures occurred at sites of metastasis. Our study’s largest limitation was that not all scans were performed on the same scanner and the doses ranged from 5 to 10 mCi approximately. We partially accounted for this difference by adjusting for the effect of the radiotracer dose, but future studies should prospectively standardize the protocol for each patient.
In our pilot study, we retrospectively evaluated fracture risk in prostate cancer patients using 18F-NaF PET/CT data. We discovered that 18F-NaF uptake could serve as an indicator of spinal bone deposition, potentially improving fracture prediction compared to existing methods like DXA. Currently, no modality can measure bone turnover rates, but 18F-NaF scans provide valuable insights into bone metabolism. This information could be clinically beneficial for predicting and preventing fractures, particularly in the context of prostate cancer. Moreover, 18F-NaF has applications in other medical fields, such as cardiac imaging for cardiovascular health assessment.[31,32] This suggests the possibility of gathering additional information about bone health during 18F-NaF PET/CT scans in aging populations, although this concept hasn’t been studied extensively yet. To advance this research, we propose that future studies explore the combination of 18F-NaF uptake with approved fracture risk assessment tools to determine its added value in fracture prediction and prevention.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






