Effect of Teriparatide on Healing of Atypical Femoral Fractures: A Systemic Review
Article information
Abstract
Background
Bisphosphonates (BPs) are the most commonly used anti-osteoporotic drugs, which have been proven to reduce the risk of osteoporotic fractures. However, use of BPs, particularly for long periods of time, is associated with an increased risk of atypical femoral fracture (AFF). Healing of BP-associated AFF is usually delayed because of suppressed bone turnover. Teriparatide (TPTD), a recombinant form of parathyroid hormone (PTH), enhances bone healing in patients with delayed healing or non-union.
Methods
In this study, we summarized and performed a systemic review of the published literature on treatment of AFF using TPTD.
Results
Although there is a lack of level 1 studies on the evidence of TPTD in promoting bone union in AFFs, this systemic review of the available literature revealed that TPTD works positively in AFFs, and we put together the evidence that TPTD is a viable treatment option for enhancing fracture healing in AFFs.
Conclusions
While anecdotal evidence of beneficial effects of TPTD on fracture healing offer limited guidance for clinical decision making, a better understanding of the role of TPTD in fracture healing may be elucidated with future prospective trials.
INTRODUCTION
Bisphosphonates (BPs) are the most commonly used anti-osteoporotic drugs, which have been proven to reduce the risk of osteoporotic fracture. BPs are also known to improve quality of life in patients with osteoporosis [1] and reduce mortality in patients who have sustained hip fractures.[2] However long term use of BPs is associated with an increased risk of atypical femoral fracture (AFF).[34] AFFs are transverse or oblique stress fractures without comminution occurring in the cortex of the subtrochanteric region or shaft of femur.[567]
Anti-resorptive agents including BPs reduce the rate of bone remodeling, therefore slowing the progression of structural loss in bone matrix. Bone matrix then undergoes more complete secondary mineralization rather than being removed and replaced with younger and less mineralized bone matrix,[8] which paradoxically makes bones more brittle because it cannot absorb energy by deformation when loaded. Subsequently, the energy applied to the bone is dissipated by micro-cracking.[9] As seen in prolonged BP administration, microcracks propagate and lengthen with less resistance in homogeneously mineralized bone matrix.[10] In addition, reduced removal of bone microdamage increases occurrence and propagation of microcracks and compromises the material strength of bone, leading to increased occurrence of stress fractures.[11]
Because of suppressed bone turnover, healing of BP-associated AFF is also usually delayed.[1213] Teriparatide (TPTD), a recombinant form of parathyroid hormone (PTH) and an anti-osteoporotic agent with potent bone-forming effects,[1415] enhances bone healing in patients with delayed healing or non-union.[16] A number of studies have demonstrated beneficial effects of TPTD on fracture healing in various animal models, both radiographically and histologically.[1718192021] However, there is only limited data for humans currently available for TPTD in fracture healing.[22] When AFF is diagnosed in a patient, the use of BPs as anti-osteoporotic drug is stopped and replaced with TPTD or a selective estrogen receptor modulator. The positive effect of TPTD on fracture healing has prompted the use of TPTP to promote the union of AFF as well.[2324] Although a number of narrative literature reviews exist elaborating on the role of TPTD in AFF, there is a lack of systematic review of the literature on the subject. In this study, we summarized and performed an in-depth review from published literature on the treatment of AFF using TPTD.
METHODS
We performed searches of PubMed, EMBASE, Web of Science, and the Cochrane Database of Systematic Reviews (CDSR) using the search terms "TPTD", "PTH", "atypical fracture", "atypical femoral fracture", and "healing." We also screened the references of the searched articles for additional information. Due to the limited amount of literature available on this topic, case reports and case series were also included in the final analysis. Exclusion criteria included articles not relevant to the use of TPTD in AFF, non-English articles, stand-alone abstracts, meeting presentations, commentaries, and review articles.
Searching the aforementioned databases yielded 72 results. Two authors independently read and reviewed the abstracts and full text of the retrieved articles. Eleven articles were deemed appropriate for our study. These included 1 article reporting results from a prospective study, 3 articles from retrospective case series, and 7 case reports. These articles were then analyzed in detail (Fig. 1).

Flow chart of article selection process.
RESULTS
Gomberg et al.[25] first reported a subtrochanteric AFF in a postmenopausal woman with a 13-year history of continuous alendronate therapy that was treated with TPTD, vitamin D, and calcium. However, thigh pain, presented as an initial symptom, intensified, and the magnetic resonance imaging (MRI) showed the appearance of fractures worsening. TPTD treatment commenced, and 6 months later, a repeat MRI showed decreased edema at the fracture sites with faint cortical bridging. Six other reports had similar findings. In all, 7 case reports with 8 patients and 11 AFFs (7 incomplete, 4 complete) were described. All the patients were elderly Asian or Caucasian females (age ranging from 63 to 84 years). TPTD treatment started at 1 to 11 months after detection of AFF. TPTD was administered for 3 to 24 months. Daily subcutaneous (SC) injection was the most common form of treatment (4 patients) although Weekly injection was used in 1 patient. Combination treatments included intramedullary nailing in acute fracture setting or as a prophylaxis (for 4 AFF cases), prophylactic locking plate (for 2 AFFs), vitamin D and calcium supplementation in 2 patients. Fracture healing was observed after 3 to 21 months after TPTD treatment. One patient was additionally treated with strontium ranelate because of persistent discomfort after 24 months of TPTD treatment. [25262728293031]
Miyakoshi et al.[32] retrospectively reviewed the medical records of 45 consecutive AFFs in 34 Japanese patients who had received oral BPs (alendronate or risedronate) for osteoporosis before AFF and had been followed for >12 months (range, 12 to 90). Thirty-seven complete or incomplete AFFs (82%) were treated surgically and 8 incomplete AFFs (18%) were treated conservatively. Based on TPTD use after fracture, these AFFs were divided into non-TPTD (n=24) and TPTD (n=21) treated groups. In subanalyses for all AFFs treated surgically, mean time to fracture healing was significantly better in the TPTD group (5.4±1.5 months) than in the non-TPTD group (8.6±4.7 months, P=0.012), and the frequency of delayed healing or non-union was significantly lower in the TPTD group than in the non-TPTD group (P=0.014). On the other hand, subanalyses for incomplete AFFs treated conservatively showed no significant differences between the groups.[32]
Saleh et al.[33] retrospectively examined 10 patients with a total of 14 incomplete AFFs. Five fractures did not have a radiolucent fracture line and were treated conservatively with partial weight-bearing restrictions and TPTD. All these fractures healed with conservative management. Nine fractures had a radiolucent fracture line, and only 2 of these were treated successfully with conservative management including TPTD. Six of 8 patients with a radiolucent line opted for surgical prophylaxis after 3 months of conservative management, whereas 1 patient underwent surgical prophylaxis without a trial of conservative management.[33]
Miller and McCarthy [34] studied 15 clinic patients with AFF who underwent quantitative bone histomorphometry both before and after 12 months of TPTD (20 µg SC/day). All patients had been on long-term alendronate (mean=7 years, range, 6 to 11 years) and had already had intramedullary rods placed when first seen (6 weeks to 7 months after rod placement). Discontinuation of BP and administration of TPTD was associated with an increase in all three dynamic histomorphometric parameters including bone formation, mineralizing surface, and mineral apposition. Baseline bone turnover markers did not correlate with the baseline histomorphometry.[34]
Chiang et al.[23] performed a prospective study involving 14 consecutive patients presenting during 2 years with AFF. All patients were offered TPTD therapy unless contraindicated. Of these 14 patients, 6 had unilateral and 8 had bilateral AFFs. Five patients agreed on the treatment with TPTD, one following a stress fracture and 4 patients because of persisting fracture non-union and ongoing pain. The remaining 9 patients (5 with complete, 4 with incomplete fractures) were not treated due to contraindications to use of TPTD. Twenty µg of daily TPTD given SC for 6 months to 5 patients was associated with a 2 to 3-fold increase in bone remodeling markers (P=0.01) and fracture healing. Of 9 patients managed conservatively or surgically without TPTD, 6 had poor fracture healing with ongoing pain, one sustained a contralateral atypical fracture, and one had fracture union after 1 year (Table 1).[23]
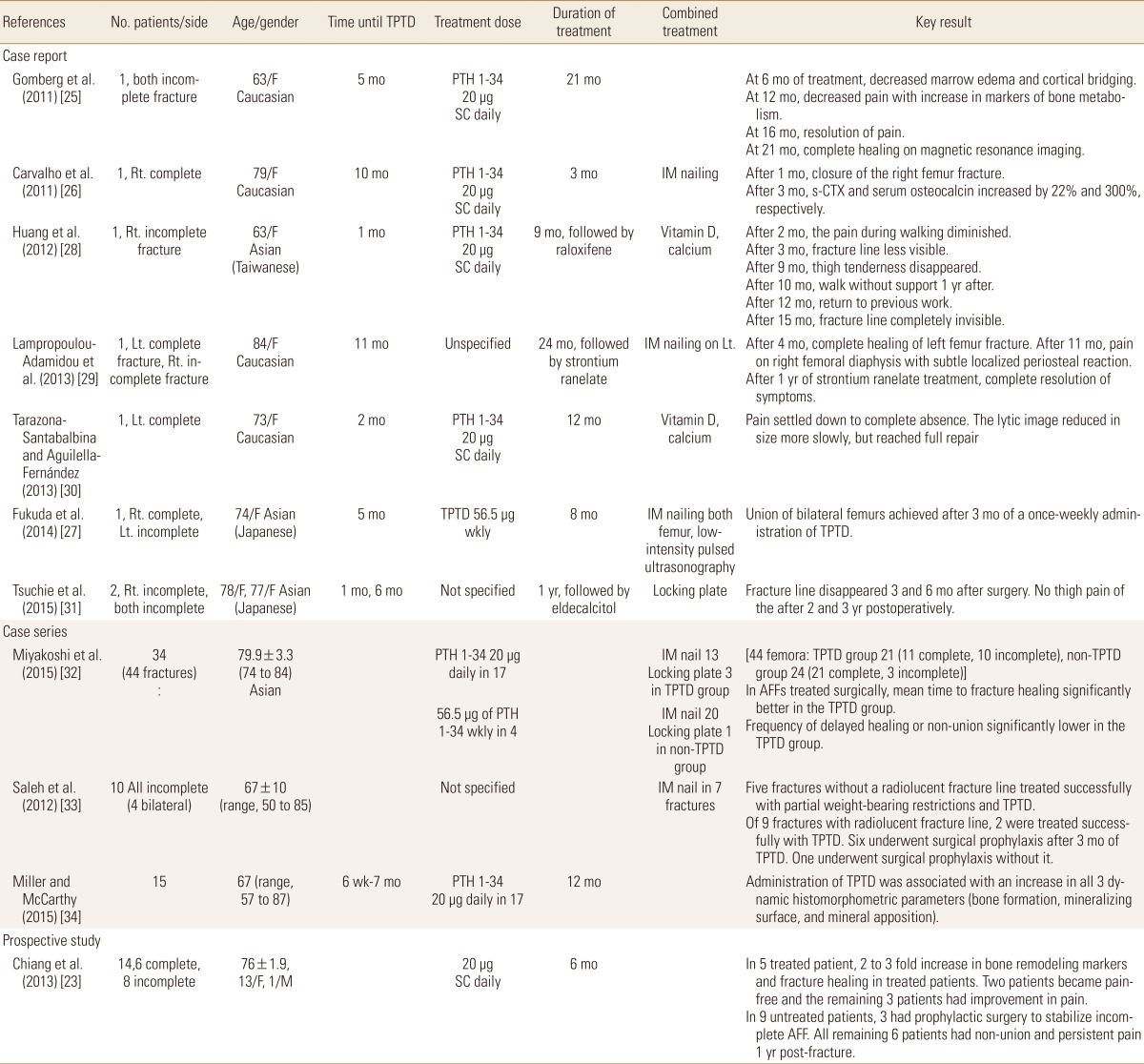
Summary of the published studies referred in the report
DISCUSSION
AFF wreaks catastrophe on osteoporotic patients who have had prolonged BP treatment. The over-mineralized fracture ends in these patients pose challenge to fracture union because of delayed bone remodeling. TPTD, which is a bone-forming agent used for nonunion, has become a key therapeutic agent for promoting bone union in AFF. A recent paper elucidates a working mechanism that can possible explain the action of TPTD in AFFs. Murphy et al. [35] employed a mixture of traceable BPs, namely fluorescent-labeled pamidronate and radiolabeled zoledronic acid in an animal study. The traceable BPs were dosed in Wistar rats for models of normal growth and closed fracture repair. Consistent with increased BP remobilization with PTH (1-34) (a form of TPTD), there was a significant decrease in fluorescence in both the long bones and in the fracture callus in PTH-treated animals compared with controls rats. Increased intracellular BP was noted in resorbing osteoclasts, confirming that, in principle, PTH (1-34) increased bone turnover as well as BP turnover.
Although there is a lack of level 1 study on the evidence of TPTD in promoting bone union in AFFs, our systemic review of the literature reveals that TPTD works positively for AFFs. Case reports continue to provide anecdotal evidence of the efficacy of PTH for fracture healing but are of limited utility in guiding clinical decision making. The prospective study of Chiang et al.[23] shows the advantages of using TPTD in AFFs that have inherent difficulty in achieving fracture healing. The results from the study of Miyakoshi et al. [32] show that TPTD administration shortens the union time and reduces the incidence of delayed or nonunion in surgically treated AFFs while it is undetermined in non-surgical cases. The series of Saleh et al.[33] shows that incomplete fractures without radiolucent lines are responsive to TPTD alone whereas those with radiolucent line needed intramedullary nailing. These results imply that TPTD works best when the fracture site is stable, either inherently or with surgical fixation.
Addressing fracture healing in AFFs is very important, and it can be achieved using anabolic therapy. We have conducted a systematic review of the literature on the use of TPTD to enhance fracture healing. Our study has the limitation of depending on the quality of the studies it analyzed. Due to limited available evidence on TPTD use for AFFs, we relied considerably on case reports and retrospective case series in this study. While anecdotal evidence of beneficial effects of TPTD on fracture healing offer limited guidance for clinical decision making, a better understanding of the role of TPTD in fracture healing may be elucidated with future prospective trials. As such, TPTD is currently a viable treatment option to enhance fracture healing in AFFs.
Notes
No potential conflict of interest relevant to this article was reported.