Paget's Disease of Bone Affecting Peripheral Limb: Difficulties in Diagnosis: A Case Report
Article information

Abstract
In terms of management of Paget's disease of bone (PDB), early diagnosis and proper management achieving remission is essential with lifelong specialist follow-up. We present the case of a 40-year-old woman with PDB affecting mainly the distal extremities (ankle and wrist). The patient visited our hospital in 2012 with heel pain. Plain radiography revealed osteoporosis, and a bone scan revealed hot uptake. Initial laboratory investigations showed normal serum calcium, 25-hydroxy-vitamin D, and parathyroid hormone levels; however, osteocalcin, C-terminal telopeptide of type I collagen, and bone alkaline phosphatase levels were elevated. A bone mineral density scan showed T- and Z-scores of −2.5 and −2.7, respectively, and bisphosphonate treatment was initiated. Biopsy performed on the calcaneal lateral wall revealed inconclusive findings. Follow-up biopsy on the left distal radius was performed 7 years later to investigate wrist pain, and this examination led to a final diagnosis as PDB. We suggest inconclusive biopsy result during the early phase of PDB and highly recommend follow-up evaluation in osteoporosis with atypical behavior.
INTRODUCTION
Paget's disease of bone (PDB) is a chronic progressive disorder, which is pathologically characterized by increased osteoclastic activity and abnormal bone formation.[1]
PDB can affect a single bone (monostotic) or multiple bones (polyostotic) and mainly involves the axial skeleton including the bones of the skull, spine, and pelvis, as well as the femur and sacrum, with only 17% invading focally.[1] This condition is uncommon in Asian countries and usually affects elderly individuals. It is unusual in individuals aged <40 years, and men are more commonly affected.[12]
The short-term treatment objectives for PDB are to reduce bone turnover and alleviate symptoms, whereas the long-term objective is to induce remission to prevent disease progression. Early use of antiresorptive therapies prevents development of deformities and arrests progression of the disease and further fractures.[34] Therefore, early diagnosis and proper management achieving remission is essential with lifelong specialist follow-up.[5]
We report a rare case of PDB in a 40-year-old Korean woman, diagnosing lately 7 years after her initial visit. She presented with involvement of multiple bones of the distal extremities. We describe the diagnosis and treatment of PDB in this case.
CASE REPORT
A 40-year-old, 166-cm-tall premenopausal woman weighing 57 kg visited outpatient clinic with gradually increasing left wrist pain for the past months without a history of trauma. Seven years prior to the visit, she had been treated with lateral impingement of the ankle secondary to a calcaneal deformity for a similar episode of worsening right heel pain. At that time, plain radiography and computed tomography of the right ankle revealed significantly reduced bone density, particularly affecting the calcaneus, suggesting osteoporosis (Fig. 1A, B). A whole-body bone scan revealed persistent high tracer uptake at the right calcaneus (Fig. 1C). Calcaneal lateral wall ostectomy and bone biopsy were performed and multifocal lesions with both osteoblastic areas and osteoclastic bone resorption were observed (Fig. 2). No conclusive diagnosis was established, and the patient was followed-up regularly for persistent right heel pain. Three years after surgery, she presented with a trivial ankle sprain and was diagnosed with an avulsion fracture of the posterior tuberosity of the right calcaneus (Fig. 3). She received conservative treatment, and a short leg cast was applied until bone union and the patient was referred to the endocrinology unit for further workup.
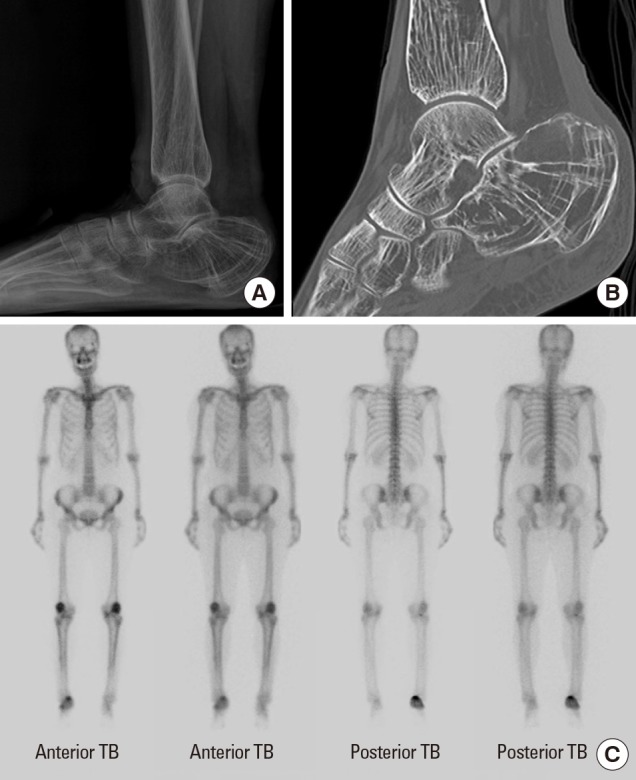
Initial imaging studies performed at the time of the patient's first visit for right heel pain. (A) A standing lateral ankle radiograph showing osteoporosis around the ankle joint. (B) A computed tomography scan (sagittal view) showing severe osteoporosis, particularly involving the calcaneus. (C) A whole-body bone scan presented increased uptake at the right calcaneus.
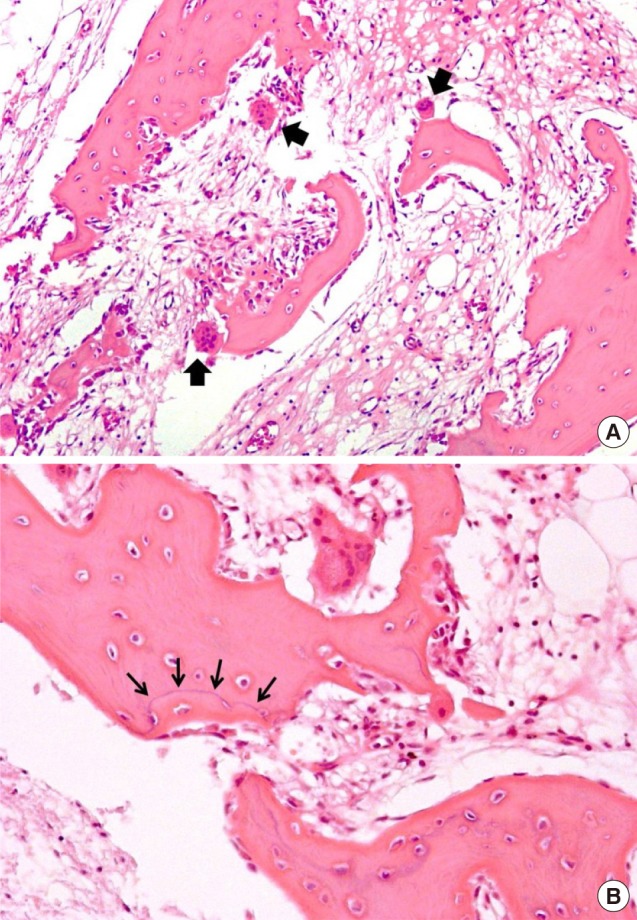
Bone biopsy result performed on right lateral calcaneal wall on May 2012. (A) Intense activation of osteoclast (arrows) showing bone resorption. Irregular thin and thick bone trabecular with osteoblastic rimming (×100). (B) Abnormal wavy cement lines were also noticed (×200).

Lateral radiograph of the ankle obtained on April 6, 2015 showing an avulsion fracture of the posterior tuberosity of the calcaneus.
Initial laboratory investigations revealed all biochemical, endocrine, rheumatology, and hematology evaluations were within normal, but serum osteocalcin, C-terminal telopeptide of type I collagen (CTX), and bone alkaline phosphatase (ALP) levels were elevated (Table 1). A bone mineral density (BMD) scan showed Z-scores of −1.3, −2.2, and −2.7, in her Lumbar 1 to 4 spines, left (Lt) femur and right (Rt) femur, respectively. The patient started ibandronate injections every 3 months on an impression of secondary osteoporosis without cause. After 1-year of treatment, her laboratory test values had returned to the normal range (Table 1), and BMD scans revealed that her Z-scores had improved to −0.5, −1.9, and −2.5, in her Lumbar 1 to 4 spines, Lt femur and Rt femur, respectively. Her heel pain was also subsided.
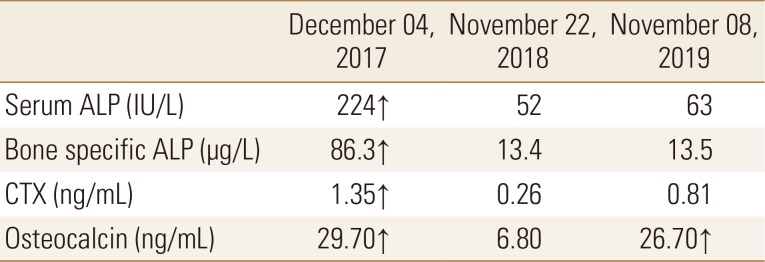
Serial follow-up serum ALP, bone specific ALP, CTX, and osteocalcin level performed on endocrinology unit
Based on previous history and a positive response to bisphosphonate therapy, PDB was sustained so bone biopsy was performed on the radial aspect of distal radius which radiograph showed osteopenia (Fig 4). Histopathological findings revealed irregular broad trabeculae with disorganized cement lines and a patchy mosaic pattern in addition to a few distinct areas of osteoclastic bone resorption and prominent osteoblastic rimming (Fig. 5). During the further evaluation, old 2nd lumbar wedge compression fracture was noticed so follow up whole body bone scan was taken 7 years after initial scan. There was still persistent uptake in right calcaneus (Fig. 6A) and plain X-ray presented bony deformity (Fig. 6B). She is still being treated with bisphosphonate with regular follow-up.

Wrist radiograph (anteroposterior view) showing diffuse osteopenia of the bone around the wrist joint.
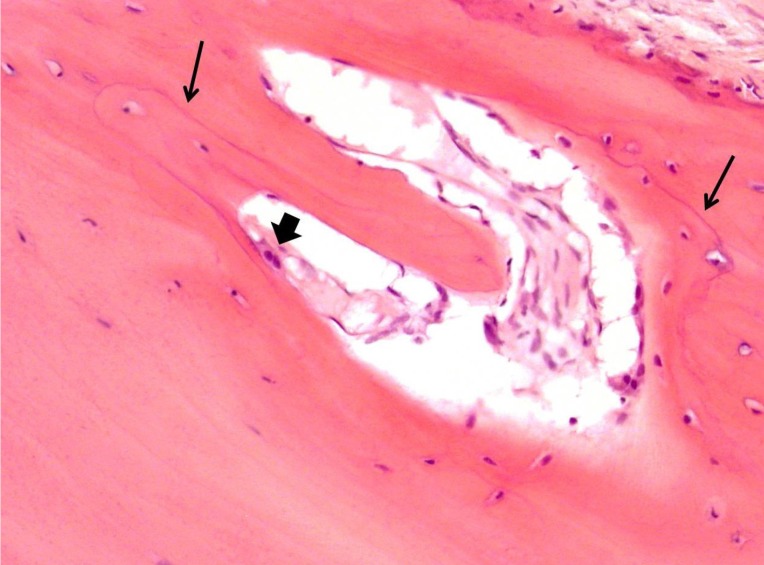
Bone biopsy done on the left radial aspect of distal radius bone on August 2019. Irregularly broad trabeculae with disorganized cement lines and patchy mosaic pattern (thin arrows), osteoclastic activity was much reduced and focally observed as with osteoblastic rimming (thick arrow) (×200).

Follow-up radiologic evaluation in 2019, whole body bone scan (A) and lateral plain X-ray of right ankle presenting bony deformity (B).
DISCUSSION
The 7-year delay in the diagnosis of PDB could be attributed to the following factors: (1) PDB commonly affects the axial skeleton and is more common in men, particularly during old age. This case was diagnostically challenging because of the unusual clinical presentation in this 40-year-old woman who presented with only calcaneal involvement on an initial bone scan. (2) Biopsy of the lateral calcaneal wall performed in 2012 was insufficient to conclusively diagnose PDB.
The PDB is the second most common bone remodeling disease after osteoporosis. Compared with low bone formation and increased bone resorption in primary osteoporosis by aging or menopause, the point DNA mutation (PDM) occurs with increased osteoclasts activity leading excessive bone resorption and subsequent osteoblasts activation with more bone formation. Therefore, the PBD is high turnover metabolic bone disease, presenting Increased biochemical indicators including osteocalcin, CTX and bone specific ALP and finally yielding abnormal weak bone remodeling.
The PDB is common in Western countries including the UK, Western Europe, New Zealand, South Africa, and South America but relatively rare in African blacks and in Southeast Asia, Korea, China, Japan, and India.[12] In fact, only a few cases of PDB have been reported, and to date, no epidemiological studies have been reported in the Republic of Korea.[678]
A positive family history is observed in approximately 15% to 30% of patients, and first-degree relatives of patients with PDB show an approximately 7-fold higher risk of PDB. Familial PDB is diagnosed in younger individuals and affects more multiple bony involvement than sporadic disease.[9] Our patient presented with right heel pain since she was in her late 30s but denied a family history of this condition.
Approximately 1% to 2% of white individuals aged >55 years may be diagnosed with PDB, and the prevalence may be as high as 25% in those aged >85 years.[10] The prevalence of PDB increases with age, and this condition is rare in those aged <25 years and unusual in those aged <40 years. Our patient developed clinical symptoms in her late 30s; however, biopsy was performed at 40 years of age. Initial histopathological examination revealed multifocal lesions comprising both osteoblastic areas and areas of osteoclastic bone resorption with abnormally high osteoclastic activity, indicating the initial osteolytic stage of PDB. However, these histopathological findings may also be observed at a usual fracture site; therefore, PDB was not conclusively diagnosed at the patient's initial evaluation. Biopsy performed 7 years after the initial evaluation revealed irregular broad trabeculae with disorganized cement lines and a patchy mosaic pattern consistent with the pathognomonic sclerotic phase of PDB.[411]
Usually, PDB mainly affects the axial skeleton; however, our patient presented with involvement of the distal extremities (the ankle and wrist), although she was also diagnosed with an old 2nd lumbar vertebral body compression fracture. Approximately 70% of patients with PDB are clinically asymptomatic and are incidentally diagnosed based on radiological findings or elevated ALP levels observed on laboratory investigations. However, some patients may present with bone pain and/or deformities and secondary arthritis. Our patient presented with vague focal pain confined to the wrist and ankle without a history of significant trauma. A previous study has described PDB affecting the radius.[12]
Several biochemical indicators of bone metabolism are useful to diagnose PDB and assess the treatment response. Serum ALP is usually elevated; notably, bone-specific ALP is a sensitive and useful marker in patients with concurrent liver disease, which can lead to serum ALP elevation. Elevation of bone-specific ALP levels reflects increased osteoblastic activity and is therefore a marker of the extent of the disease.[413] The bisphosphonate class of drugs such as alendronate normalize bone metabolism and restore the normal lamellar structure of affected bones.[1415] In our patient, elevated bone ALP (86.3 IU/L) levels returned to the normal range (13.4), and the BMD also slightly improved (T- and Z-scores of −2.5 and −2.7, respectively improved to −2.2 and −2.5, respectively), a year after ibandronate treatment.
Possible complications with PDM are hearing loss, osteoarthritis, bowing of lower extremity, paralysis, neoplasm, and congestive heart failure.[4] Many of clinical features and complications of PDB are thought to be from abnormalities of bone remodeling.[13] Early diagnosis, proper management achieving remission, and preventing above complications are essential with lifelong specialist follow-up.[345] During 7 years of diagnosis, the patient experienced calcaneal fracture and finally left bony deformity after union.
In conclusion, we present the case of a 40-year-old woman with PDB mainly affecting her distal extremities. Follow-up biopsy of the affected bones performed 7 years after initial evaluation led to a conclusive diagnosis. We suggest inconclusive biopsy result during the early phase of PDB and highly recommend follow-up evaluation in osteoporosis with atypical behavior.
Notes
Ethics approval and consent to participate: This study was conducted in accordance with the principles of the Declaration of Helsinki, and all patients provided written informed consent prior to enrollment.
Conflict of interest: No potential conflict of interest relevant to this article was reported.