The Association between Urine Albumin to Creatinine Ratio and Osteoporosis in Postmenopausal Women with Type 2 Diabetes
Article information
Abstract
Background
Osteoporosis is a progressive bone disease that is characterized by a decrease in bone mass density and destruction of microstructure, which can lead to an increased risk of fracture. Although many studies have been published about the relationship between end-stage renal disease and osteoporosis, research on the relationship between proteinuria and the prevalence of osteoporosis is still lacking.
Methods
We assessed 91 postmenopausal women with type 2 diabetes who visited our hospital from January 2009 to January 2012.
Results
Among 91 patients, the prevalence of osteoporosis and osteopenia was 35.2% (32 cases) and 32.9% (30 cases) according to bone mineral density. The patients with microalbuminuria and macroalbuminuria (urine albumin-to-creatinine ratio [UACR] ≥ 30) had a significantly higher incidence of osteoporosis compared to subjects with normoalbuminuria (P<0.05).
Conclusions
This study indicates that UACR may be a useful biomarker for increased risk of osteoporosis in postmenopausal women with type 2 diabetes who have been linked to higher UACR levels.
INTRODUCTION
Osteoporosis is a systemic skeletal disease characterized by abnormalities in bone structures and decreased bone density. As a result, bones become vulnerable to fractures, as defined by the World Health Organization (WHO),[1] which limits the active lives of half the osteoporosis patients older than 50 years and most patients older than 70 years.
There are various methods for diagnosing osteoporosis; measuring the bone mineral density (BMD) is the most effective standard procedure. The bone density helps identify the appropriate treatment options and is used to assess the treatment response.[12] The bone density of the lumbar spine and the femur of postmenopausal women is measured with dual energy X-ray absorptiometry (DXA) and is interpreted as normal if the lowest T-score is higher than -1.0, osteopenia if between -1.0 and -2.5, and osteoporosis if it is less than -2.5.[1]
Among the various mechanisms of osteoporosis, the absence of estrogen in postmenopausal women may be one of the major risk factors for accelerated bone loss.[3] Additionally, decreased BMD and an increased risk for fractures have been reported in patients with type 1 diabetes mellitus (DM). However, patients with type 2 DM are known to have various changes in the BMD and an increased risk of fractures from falls.[456]
According to the Korea National Health and Nutrition Examination Survey held in 2012, the prevalence rate of osteoporosis in women older than 50 years was 4 times higher than in men the same age (34.9% vs. 7.8%).[7] The frequency of osteoporosis sharply increased due to the decreased production of estrogen after menopause and with aging.[8] Although patients with type 2 DM had normal or increased BMD of the lumbar spine, head of the femur, and hipbone even after body mass index (BMI) calibration,[910] a meta-analysis showed that patients with type 2 DM had increased risk for fracture of the femur.[11]
In addition, chronic nephropathy is reported to affect bone metabolism.[121314] In this study, we investigated the relationship between osteoporosis (determined by BMD), the estimated glomerular filtration rate (eGFR), the computation of the creatinine clearance (CCr), and the urine albumin-to-creatinine ratio (UACR) as an overall index of kidney function in menopausal women with type 2 DM.
METHODS
1. Subjects
From January 2009 to January 2012, the study was conducted on 91 postmenopausal women >50 years of age (mean age, 55.4±6.3 years; range, 45 to 74 years) with type 2 DM who were confirmed in the department of internal medicine. Postmenopausal status was defined as more than one year of amenorrhea, or age older than 50 years for women who had had a hysterectomy.[15] We defined type 2 DM in accordance with the criteria of the Korean Diabetes Association.[16] Patients were excluded from this study if they had a history of thyroid, parathyroid, oligomenorrhea, or amenorrhea before 40 years, hyperprolactinemia, oophorectomy, rheumatoid arthritis, ankylosing spondylitis, malabsorption syndromes, malignant tumors, hematologic diseases, previous pathological fractures and traumatic fractures or those patients with serum creatinine (Cr) levels greater than 2.0 mg/dL. The protocol for this study was approved by the Ethics Committee at Dongsan Medical Center and signed informed consent was obtained from each participant.
2. Methods
A detailed questionnaire was completed by each of the 91 participating patients. Information obtained included age, gender, height, weight, smoking history, history of alcohol consumption, duration of DM, and history of hypertension or cardiovascular diseases. Additionally, baseline laboratory data including fasting blood glucose (FBG), glycosylated hemoglobin (HbA1c), serum total bilirubin, aspartate aminotransferase (AST), alanine aminotransaminase (ALT), Cr, and lipid profiles were analyzed. For all participants, BMD at the lumbar and hip region were measured by DXA, it is interpreted as normal if the lowest T-score is higher than -1.0, osteopenia if between -1.0 and -2.5, and osteoporosis if it is less than -2.5. Renal function was estimated by eGFR with a Modification of Diet in Renal Disease (MDRD) equation,[17] CCr with a Cockcroft-Gault equation, [18] and the UACR.[19] Albuminuria was defined as UACR 30 to 300 mg/g as microalbuminuria and UACR ≥300 mg/g as macroalbuminuria.[20]
3. Analysis
Statistical analysis was performed using SPSS version 21.0 (SPSS Inc., Chicago, IL, USA) and the baseline characteristics of participants were presented as the mean±standard deviation and n (%). Multiple regression analysis was performed to assess independent associations between key risk factors and BMD. The prevalence of osteoporosis and osteopenia in microalbuminuria and macroalbuminuria groups was analyzed by Chi-square test. A P-value of less than 0.05 was considered statistically significant.
RESULTS
1. Clinical characteristics of the patients
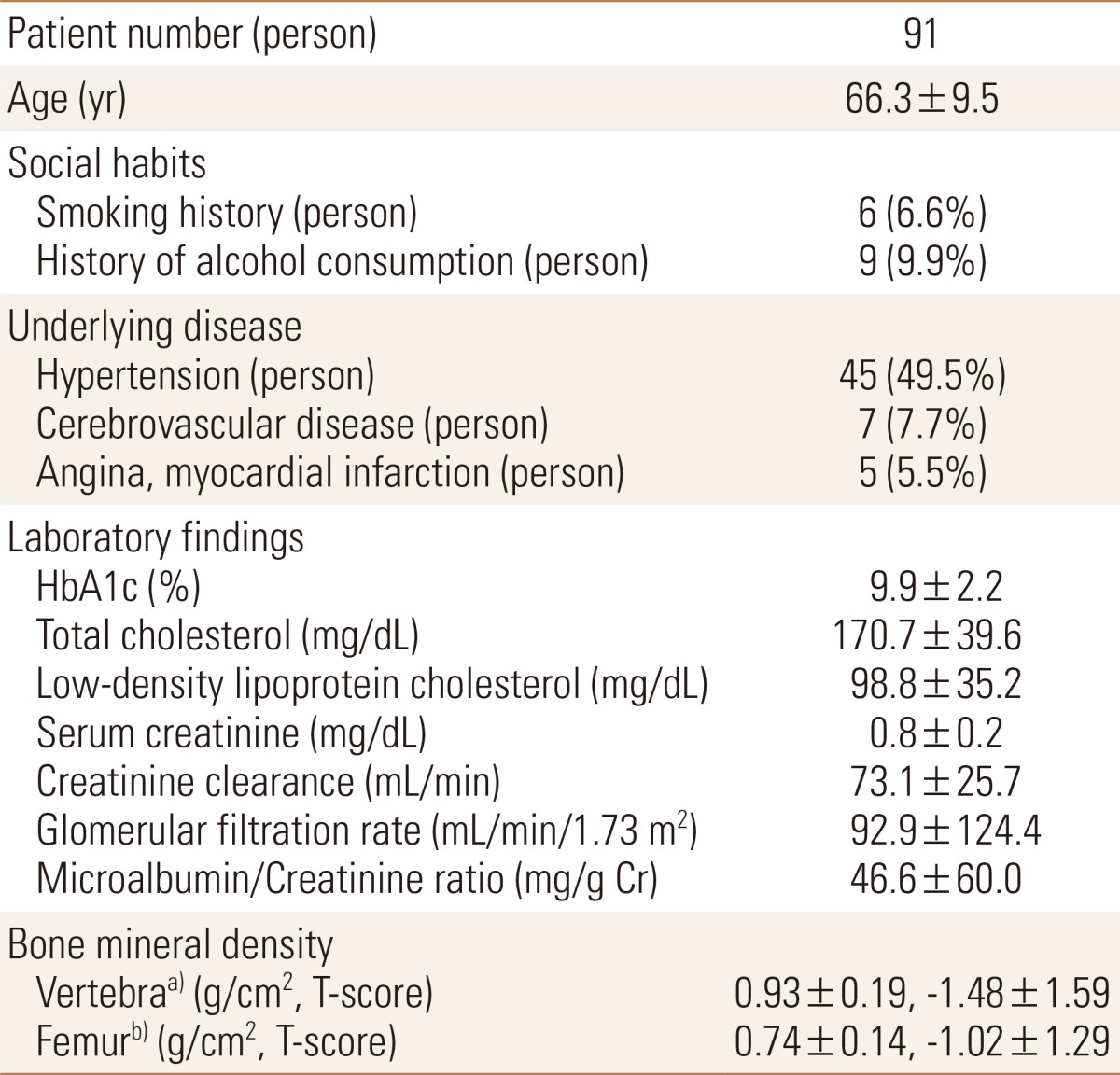
The baseline clinical and laboratory characteristics of the study population are shown in Table 1. Among the participants, the mean age was 66.3 years and BMI was 24.8 kg/m2. The duration of DM was on average 11.5 years. The laboratory data showed a mean HbA1c of 9.9% and osteoporosis 35.2% (32 cases). Renal function of the patients was estimated by eGFR, CCr, and UACR and mean eGFR, CCr, and UACR were 92.9 mL/min/1.73 m2, 73.1 mL/min, and 46.6 mg/g Cr. The prevalence of albuminuria ≥30 mg/g Cr was 38.5% (35 cases).
Comparison of patients groups at the time of admission
2. The relationships between BMD and the clinical conditions
The analysis was performed using a multiple regression analysis of the association between vertebral BMD and each independent variable, statistically significant results were obtained as a result, showing a statistically significant probability of less than 0.05 between age, BMI, CCr and vertebral BMD. The calibration coefficient of the determination R2 value was 0.412, and the explanatory power of the model was also relatively high. In the regression coefficient, the age regression expression was -0.006 and depending on the age increase in the subjects, vertebral BMD showed a decrease. Each regression coefficient of BMI and CCr was 0.009 and 0.003, respectively. Increased vertebral BMD was dependent upon increases in both BMI and CCr in the subjects (Table 2).
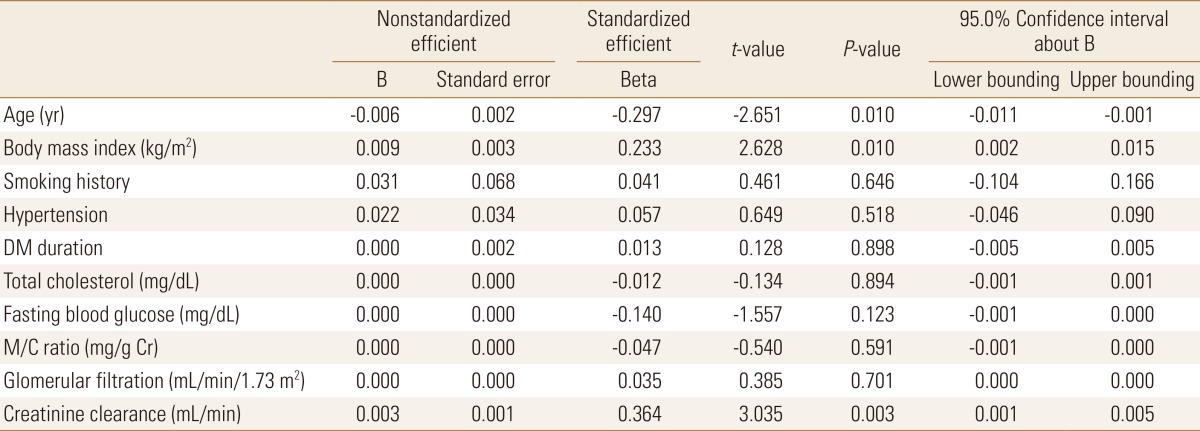
The association between vertebral bone mineral density and each independent variable
Also, the analysis was performed using a multiple regression analysis of the association between BMD of the femur and each independent variable. Each of the independent variable and BMD of the femur were obtained only by age specific statistically significant results that showed a statistically significant probability of 0.01. The calibration coefficient of the determination R2 value was 0.494, and the explanatory power of the model was also relatively high. In the regression coefficient, the age regression expression was -0.008 and depending on the age increase in the subjects, BMD of the femur showed a decrease. Each regression coefficient of BMI and CCr was 0.006 and 0.002, respectively. Increased BMD of the femur was dependent upon increases in both BMI and CCr in the subjects (Table 3).
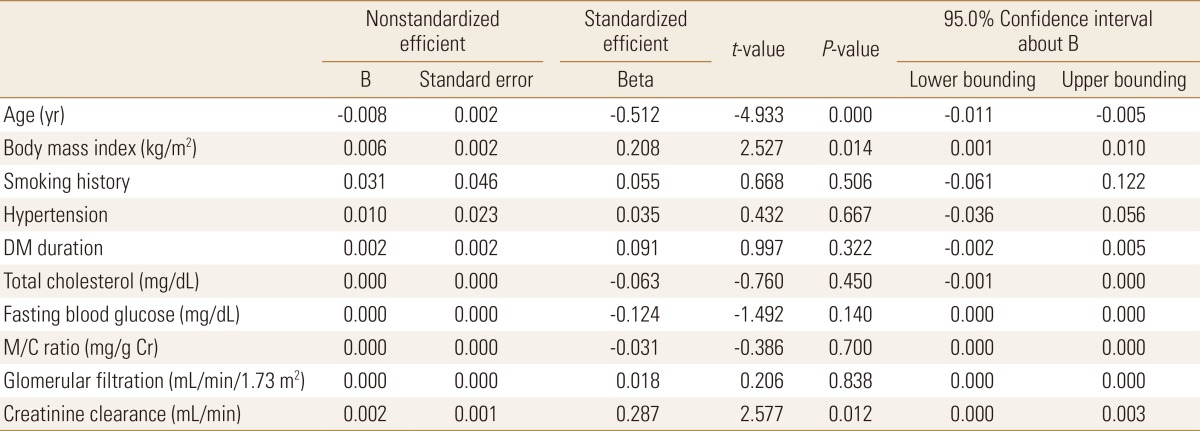
The association between bone mineral density of the femur and each independent variable
In addition, the analysis was performed using a multiple logistic regression analysis of the association between two groups according to the results of BMD and each independent variable. Groups were divided into normal and abnormal consisted of patients with osteopenia and osteoporosis based on the result of BMD. Statistically significant results were obtained as a result, showing a statistically significant probability of less than 0.05 between age, smoking history, CCr and two groups according to the results of BMD (Table 4).
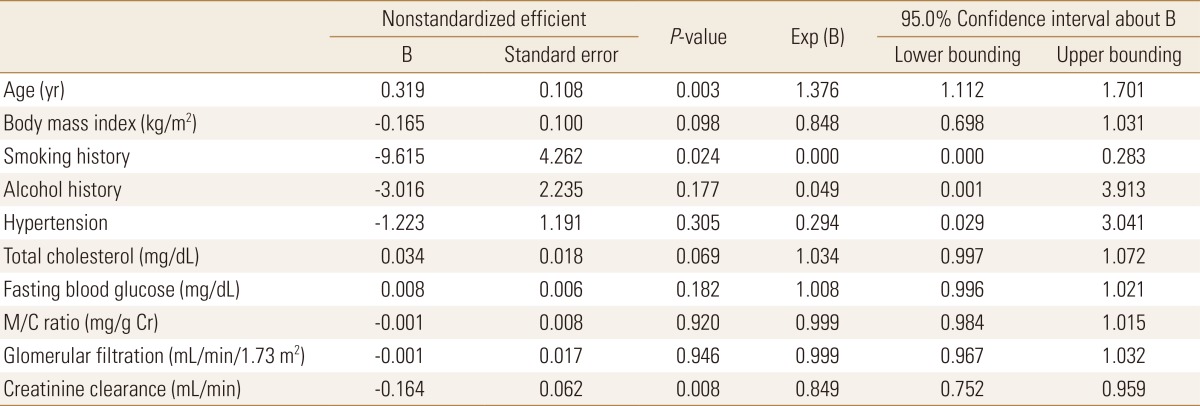
Multiple logistic regression analysis of the association between two groups according to the results of bone mineral density and each independent variable
3. The prevalence of osteoporosis according to albuminuria
The prevalence of osteoporosis according to the clinical conditions was estimated (Table 5). The patients with albuminuria (UACR ≥30 mg/g Cr) had a significantly higher prevalence of osteoporosis (51.4%) compared to patients with normoalbuminuria (UACR <30 mg/g Cr, P<0.05).

Prevalence difference of osteopenia and osteoporosis according to the proteinuria
DISCUSSION
Although several studies have reported an association between DM and the high risk of pathological fractures, the relationship between DM and osteoporosis remains controversial.[21] Recent studies have reported an association between type 1 DM and reduced BMD, while patients with type 2 DM generally have modestly increased or unchanged BMD.[5] Given the discrepancies between BMD and fracture rate, there may be other clinical factors affecting new bone formation, bone microarchitecture, bone quality, or BMD in DM. Patients with DM may have lower bone quality resulting from several mechanisms including hyperinsulinemia, the deposition of advanced glycosylation end products (AGEs) in collagen, reduced serum levels of insulin-like growth factor-1 (IGF-1), hypercalciuria, microangiopathy, inflammation, and renal failure.[5]
The kidney is an important organ for regulating calcium and phosphorous metabolism, not only as the target organ for parathyroid hormone (PTH), but also a principal site for calcitriol (1,25-dihydroxy-vitamin D [1,25-(OH)2D]) production.[22] The association between chronic kidney disease and reduced BMD and the resulting increased risk of fracture is well recognized.[2324] In chronic renal failure (CRF) with an eGFR below 60 mL/min, phosphate is retained inducing a rise in the PTH and a decline in 1,25-(OH)2D levels. Therefore, bone disease such as renal osteodystrophy is observed in 75 to 100% of patients with CRF due to abnormal bone turnover, coupling, and mineralization.[25] In patients with further reduction in the eGFR to 20 to 40 mL/min, skeletal PTH resistance also increases with worsening uremia and patients have abnormal bone histology with impaired calcium and phosphate homeostasis.[26]
The number of patients with CRF is rapidly increasing and the most common primary cause of CRF identified in Korea was diabetic nephropathy (45.4%).[27]
The GFR is traditionally considered the best overall index of kidney function and has been estimated by the measurement of serum Cr and Cr excretion in a 24-hr urine sample and computation of the CCr.[28]
In patients with type 2 DM, the annual evaluation for albuminuria is recommended in order to monitor for disease progression and response to therapy. A spot UACR, preferably in a first-morning void, correlates well with a 24-hr urine albumin excretion rate and accurately predicts renal events. Because of convenience, the UACR test has been utilized as the first-line annual screening test for patients with type 2 DM.[29]
Microalbuminuria is a strong and independent marker of increased cardiovascular risk.[30] A common pathophysiologic process, such as endothelial dysfunction probably explains the association between microalbuminuria and cardiovascular disease.[30] In addition, endothelial dysfunction of the glomerular basement membrane can modify the glomerular barrier permeability of the kidneys, facilitating the urinary excretion of albumin.[31] An early stage in the development of atherosclerosis, endothelial dysfunction reduces the bioavailability of nitric oxide.[32] As albuminuria is associated with endothelial dysfunction and damage, it may also play a key role in the development of atherosclerosis.[33] Furthermore, several studies have demonstrated the effect of atherosclerosis on the BMD and bone metabolism.[34353637] Pathophysiological mechanisms between atherosclerosis and osteoporosis are complex.[38] During atherosclerosis, the increase in the serum levels of some inflammatory cytokines such as C-reactive protein, interleukin-6 (IL-6), and tumor necrosis factor-α confirms the inflammatory etiology of osteoporosis.[39] These inflammatory cytokines are potent stimulators of bone resorption.[39] The bone resorptive potential of monocytes has been directly correlated to serum IL-1, IL-6, and tumor necrosis factor-α levels in postmenopausal women. [40] In addition, these cytokines stimulate the proliferation and differentiation of osteoclast precursors, which lead to loss of bone mass.[40] Albuminuria and BMD appear to have a strong relationship when combined, and contribute to the development of osteoporosis.
In this study, the factors affecting vertebral and femoral BMD included age, BMI, and CCr. Micro- or macro-albuminuria as measured with the UACR, was significantly associated with osteoporosis compared to normoalbuminuria. This means that the increase in UACR a recent renal evaluation marker may be significantly associated with the risk of osteoporosis in postmenopausal women with type 2 DM. A higher rate of osteopenia was demonstrated in patients with a UACR of less than 30 mg/g Cr. However, this high rate of osteopenia is believed to be due to low rate of osteoporosis. It was classified according to GFR, there was not a statistically significant result. Because both UACR and GFR is associated with kidney, it seems there is no sense to divide the GFR alone. According to the results of multiple logistic regression analysis, there was significant correlation between CCr among kidney markers and two groups according to the results of BMD. However, there was no significant correlation between UACR and two groups according to the results of BMD. This is a limitation of this study, an additional prospective study involving a large population is needed.
There are several design features and limitations in this study. First, because the subjects were postmenopausal women with type 2 DM, estrogen deficiency and DM might affect BMD or the incidence of osteoporosis. However, we were unable to evaluate the estrogen level or medication. Second, we recruited patients with serum Cr level of less than 2.0 mg/dL to detect early fracture risk in study subjects. Third, we did not evaluate bone turnover markers. Finally, this study was based on a cross-sectional study, an additional prospective study involving a large population is needed. In conclusion, this study demonstrated that urine ACR might be a useful biomarker for increased osteoporosis risk in postmenopausal women with type 2 DM.
Notes
No potential conflict of interest relevant to this article was reported.