



INTRODUCTION
Sarcopenia is a geriatric syndrome defined by a progressive impairment of muscle function due to the loss of skeletal muscle mass.[1-6] Sarcopenia increases the risk of falling and is associated with osteoporosis and hip fracture.[7,8] Compared with hip fracture patients without sarcopenia, those with sarcopenia accompanied more pain after surgery, had decreased compliance with weight-bearing, and resulted in a higher rate of physically and functionally deficient state.[9,10] Therefore, sarcopenia is one of many problems requiring treatment in elderly patients with hip fractures.
There have been various reports on the results of nutritional support and specific exercise or rehabilitation in sarcopenia patients.[11,12] Nutritional support and exercise appear to be effective in preventing or treating sarcopenia. However, the protocols of nutritional and rehabilitation interventions are different for each study, and it is difficult to determine the effectiveness depending on the characteristics of the group.[1] Also, research on whether treatment for sarcopenia is effective in elderly hip fracture patients with reduced digestive or cognitive function is scarce.[2] Nevertheless, sarcopenia is an important factor influencing the outcome of treatment for hip fracture patients, thus, a study on effective treatment is essential.[2]
Therefore, the purpose of this study is to (1) investigate nutritional or rehabilitation intervention protocols; and (2) to analyze the effect of these protocols through a systematic review of studies that report on clinical results of hip fracture patients with sarcopenia.
METHODS
Our current systematic review was performed according to the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guideline.[13]
1. Study eligibility criteria
Studies were selected based on the following criteria: (1) study design: randomized controlled trials (RCTs) or non-randomized comparative studies; (2) study population: patients with hip fracture; (3) intervention: nutritional or rehabilitation intervention; and (4) reporting the clinical outcomes and definition of sarcopenia. Studies were excluded if they failed to meet the criteria.
2. Search methods for identification of studies
A comprehensive search of all relevant RCTs and comparative studies was conducted through PubMed Central, OVID Medline, Cochrane Collaboration Library, Web of Science, EMBASE, KoreaMed, and AHRQ, up to April 2021, with English language restriction. We used the following search terms:((“sarcopenia”[MeSH Terms] OR “sarcopenia”[All Fields]) AND (“hip fractures”[MeSH Terms] OR (“hip”[All Fields] AND “fractures”[All Fields]) OR “hip fractures”[All Fields] OR (“hip” [All Fields] AND “fracture”[All Fields]) OR “hip fracture”[All Fields])). A manual search of possibly related references was also conducted. Two investigators independently reviewed the titles, abstracts, and full texts of all potentially relevant studies, as recommended by the Cochrane Collaboration.[14]
3. Data extraction
The following data were extracted from the included articles: authors, publication date, study design, characteristics of the participants, follow-up period, specific interventions, and outcome measurements.
4. Methodological quality assessment
Two authors independently assessed the methodological quality of included studies using the same criteria for RCTs and as described in the Cochrane Handbook for Systematic Reviews of Interventions 5.2. The criteria include the following: (1) Allocation concealment; (2) Were the inclusion and exclusion criteria clearly defined?; (3) Were the outcomes of patients who withdrew or were excluded after allocation described and included in an intention-to-treat analysis?; (4) Were the groups well-matched with appropriate covariate adjustments?; (5) Did the surgeons have experience in the operations performed in the trial, prior to its commencement?; (6) Were the care programs other than the trial options identical?; (7) Were all the outcome measures clearly defined in the text with a definition of any ambiguous terms encountered?; (8) Were the outcome assessors blinded to assignment status?; (9) Was the timing of outcome measures appropriate?; and (10) Were follow-up losses reported and if so, were they less than 5% of participants lost from follow-up?
The Newcastle-Ottawa scale was used to assess the methodological quality of non-randomized studies. The scale contains 8 items, which are categorized into 3 dimensions: the selection of the study population, the comparability of the groups, and the ascertainment of the exposure (case-control study) or outcome (cohort study). Each dimension consists of subcategorized questions: selection (a maximum of 4 stars), comparability (a maximum of 2 stars), and exposure or outcome (a maximum of 3 stars).[15,16] Apparently, a study can be awarded a maximum of 9 stars, which indicates the highest quality. In the present study, 2 authors independently evaluated the quality of all the studies.
RESULTS
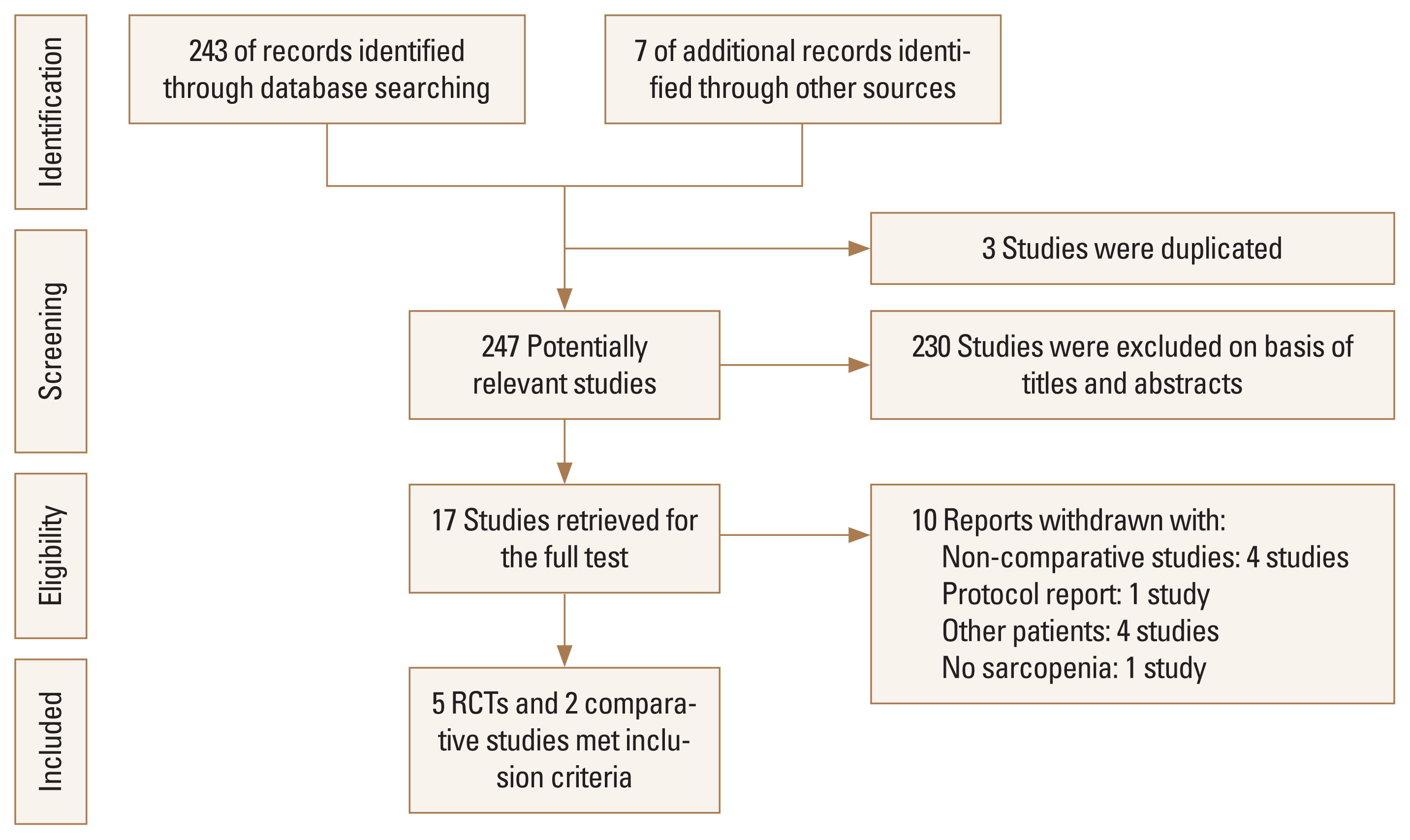
The initial search identified 247 references from the selected databases. The 203 references were excluded by screening the abstracts and titles for duplicates, unrelated articles, case reports, systematic reviews, and non-comparative studies. The remaining 17 studies underwent full-text review and subsequently, 10 studies were excluded. The details of the identification of relevant studies are shown in the flow chart of the study selection process (Fig. 1). Five RCTs and 2 comparative studies were selected for further investigation. The total number of patients was 497 (RCTs, 279; comparative studies, 221). Five studies included patients ≥65 years of age, and 2 studies included patients ≥60 years of age. There were 3 studies that applied the Asian working group criteria for the definition of sarcopenia.[2,3,17]
The main characteristics and outcomes of the studies included in this systematic review are presented in Table 1. [1-5,8,17] Two studies conducted specific rehabilitation intervention and 1 study conducted intervention using erythropoietin drugs.[2,3,17] Oh et al. [3] applied an antigravity treadmill combined with conventional rehabilitation to hip fracture patients. Antigravity treadmill was applied with 50% to 60% of body weight administered at a rate of 1.5 mph for 20 min based on a weekday. After that, the proportion of body weight and speed of the antigravity treadmill was increased step by step. Lim et al. [17] analyzed the effect of the fragility fracture integrated rehabilitation management (FIRM) program. The FIRM program consists of 10 days of physical therapy (2 60-min sessions per day), 4 days of occupational therapy, fall prevention education, discharge planning, and referral to community-based care during the-2 week hospital stay after surgery. Zhang et al. [2] administered intravenous erythropoietin to intertrochanteric fracture patients for 10 days after surgery.
Four studies conducted nutritional interventions using amino-acid or protein, although there were differences in composition, dose, and duration of intervention.[1,4,5,8] Malafarina et al. [8] provided supplements consisting of protein-fat carbohydrates, and Flodin et al. [5] provided protein with calcium and vitamin D for sarcopenia patients. In the studies of de Sire et al. [4] and Invernizzi et al. [1], patients received a 2-month amino acid supplementation.
The most frequently used assessment tool for intervention was handgrip strength (Table 2).[1-5] In addition, ambulatory functions such as the Koval score, timed up and go, body composition measured by dual energy X-ray absorptiometry, and appendicular skeletal muscle mass was used. Among the studies included in this systematic review, 2 studies did not find a clear statistical difference in assessment tools compared to controls after intervention.[4,5] However, the rest of the studies positively interpreted the effect of results for intervention. The Newcastle-Ottawa scale was used to assess the quality of the selected studies. All included studies scored 6 to 8 points, indicating relatively high quality.
DISCUSSION
Approximately 40% of elderly people with a fracture do not recover their previous functional status.[18] Functional loss is associated with institutionalization and increases mortality.[18] Bed confinement and the reduced mobility of hospitalized elderly patients are associated with loss of muscle mass and function.[19] In addition, age-related muscle loss occurs in elderly patients.[5] It has been reported that about 5% to 6% of muscle loss occurs within 1 year after hip fracture.[20] Thus, the prevalence of sarcopenia in elderly patients with hip fractures is up to 54%.[21]
The pathogenesis of sarcopenia is linked to an alteration of the homeostasis between protein anabolism and catabolism in the muscle tissue, resulting in the progressive reduction of the muscle mass.[22] This homeostasis is affected by several factors. Inflammatory cytokines, cortisol, myostatin, and the over-expression of the ubiquitin-proteasome pathway promotes muscle tissue degradation, while adequate protein or amino acid intake, growth hormone, and insulin growth factor-1 promote the synthesis of new muscle tissue.[22] Thus, mainstream methods of intervention for sarcopenia include nutritional intervention, exercise intervention and drug intervention.[2]
1. Results and limitations of studies related to rehabilitation
Oh et al. [3] applied an antigravity treadmill combined with conventional rehabilitation for 10 days after surgery in hip fracture patients with sarcopenia. Although functional scores, such as Koval score and Berg Balance Scale, improved at postoperative 3 to 6 months, they plateaued in the subsequent period. They concluded that rehabilitation with an antigravity treadmill provided additional benefit to hip fracture patients, but there is no improvement in handgrip strength. Lim et al. [17] operated an elaborate rehabilitation program for about 10 days on patients who underwent hip fracture surgery and reported the following clinical results. They insisted that the ambulatory function, assessed through Koval score, Functional Ambulatory and Category scale, of the patients investigated up to 6 months after surgery was improved by this rehabilitation program regardless of the presence of sarcopenia. However, no significant improvement in handgrip strength was observed in this study as well.
Although improvement in functional score was observed in both studies, several factors could be considered for the fact that there was no change in handgrip strength, an index related to sarcopenia. First, exercise for 10 days after surgery is considered too short to improve sarcopenia. In Lim et al.’s study [17], even considering the degree of complication due to hip fracture, 61.5% to 70% of patients who recovered to their pre-injury (fracture) ambulatory function still displayed muscle loss. Moderate to high-intensity resistance exercises can improve muscle mass and strength, and improve body muscle function.[2] We believe that additional research is needed on the intensity and duration of exercise that can increase muscle mass in hip fracture patients, and a change in rehabilitation protocol is required in consideration. Second, it is possible that the failure of social or familial support for rehabilitation after surgery may have affected the patients’ sarcopenia status. Third, there was no support for nutritional status in both studies.
2. Results and limitations of studies related to nutrition
In the studies of de Sire et al. [4] and Invernizzi et al. [1], 2 months of amino acid supplementation were performed. The main components of the amino acids used were l-leucine, l-lysine, and l-valine, with addition of vitamin B6 and vitamin B1. In the study by Malafarina et al. [8], patients were supplemented with 2 bottles per day of β-hydroxy-β-methylbutyrate (HMB), a metabolite of leucine, during hospitalization. In the study of Fitschen et al. [23], HMB has been shown to improve the synthesis and reduce the degradation of muscle proteins. The endogenous output of HMB reduces with age and its levels are associated with the loss of appendicular lean mass and handgrip strength.[24] In the study of Kuriyan et al. [24], supplementation with HMB prevents muscle loss associated with bed confinement. Branched-chain amino acids, such as leucine, are responsible for the activation of muscle metabolism by stimulating the mammalian target of rapamycin.[25]
De Sire et al. [4] measured serum myostatin levels after amino acid supplementation, but myostatin levels decreased regardless of intervention, and there was no difference between the 2 groups. Invernizzi et al. [1] reported that handgrip strength, Timed Up and Go test, and Iowa Level of Assistance scale was improved only in hip fracture patients with sarcopenia among patients who received nutritional support, but in patients without sarcopenia, improvement was not observed. In the study of Malafarina et al. [8], the intervention group undergone HMB supplementation lost weight at discharge compared to the time of admission, but to a lesser degree compared to the control group. The appendicular lean mass did not decrease in the intervention group compared to at the time of hospitalization.
The low concentration of vitamin D is associated with a reduction in muscle mass and strength, and supplementation with vitamin D is effective in the prevention and management of frailty.[26] In the studies of Artaza-Artabe et al. [26] and Flodin et al. [5], calcium and vitamin D was included in nutritional supplements. Interestingly, in the study of Flodin et al. [5], although protein-rich nutritional supplementation positively affects handgrip strength and quality of life, there was no difference in change in fat-free mass index and handgrip strength between the control group (only calcium and vitamin D) and the intervention group (calcium and vitamin D, protein, and risedronate). Also, the period of nutritional supplement was 6 months. As far as we know there have not been any nutritional intervention trials persisting longer than six months for hip fracture patients. Two possible explanations for the lack of significant benefits may be that: poor nutritional state prior to hip fracture; prolonged catabolic state, in which metabolic, hormonal, and inflammatory response to injury and operation result in an accelerated breakdown of muscle protein.[27-29]
In the studies of de Sire et al. [4] and Invernizzi et al. [1], the duration of rehabilitation was 2 weeks, and in the study of Malafarina et al. [8], exercise was performed for 5 days per week during hospitalization. A study by Flodin et al. [5] reported that conventional rehabilitation aimed at restoring the ability to walk was performed, but did not describe how long it was performed. Although nutrients and, in particular amino acids, play a key role in muscle metabolism and functioning in older people, all studies performed nutritional support and rehabilitation simultaneously. All studies reported that nutritional intervention reduced muscle mass loss, but it does not seem to completely prevent muscle mass loss, because of the short-term intervention. In addition, since the rehabilitation and nutrition protocols, methods for evaluating the effectiveness of interventions differed for each study, thus it was not possible to conclude which method was the most effective.
3. Results and limitations of studies related to medication
Patients’ comorbidity and cognitive impairment will worsen over time after hip fracture. In addition, complications of hip fracture, and pain caused by fracture itself and following surgical interventions interfere with ambulation. These can make rehabilitation or exercise difficult to sustain. Even if long-term nutritional support is provided, if continuous rehabilitation is limited, the effectiveness of nutritional support seems to be also limited. Therefore, although there is no drug proven to date, it is necessary to develop a drug that can directly affect myocytes. Erythropoietin has been reported to have therapeutic effects such as anti-apoptosis, anti-oxidation, anti-inflammation and maintenance of vascular structure, as well as a normal function.[30-32]
Zhang et al. [2] administered erythropoietin to intertrochanteric fracture patients over 60 years after surgery by classifying groups according to the presence or absence of sarcopenia and sex. They reported that erythropoietin increased handgrip strength in sarcopenic women compared to the control group, although there was no effect in sarcopenic men. They also reported that the appendicular skeletal muscle increment of the intervention group was markedly increased regardless of sex. Therefore, they insisted that erythropoietin can improve the muscle strength of female patients with sarcopenia during the perioperative period and increase muscle mass both of women and men, with erythropoietin possibly improving the symptoms of sarcopenia. Moreover, even more surprising in the study was that administration of erythropoietin reduced postoperative complications and length of stay. However, in this study, muscle strength increase due to erythropoietin was not observed in men, and they did not evaluate the reduction state of the fracture, the leg length discrepancy caused by the collapse of the fracture site, and postoperative ambulatory state. In addition, since cost effectiveness and safety for complications by erythropoietin have not been proven, caution is needed in the use of erythropoietin.
There are limitations to our study. First, because the characteristics of patients included, such as race and age, are heterogenous, the definition or measuring methods for sarcopenia in each study are different. Therefore, it may be difficult to use the protocols introduced in this study in general. Second, because the number of studies that performed intervention for the treatment of sarcopenia in patients with hip fracture was small and there were many differences between the protocols, we could not find proper intervention protocol for sarcopenia in patients with hip fracture. It is considered that further research is needed in the future.
CONCLUSION
Although mainstream methods of intervention for sarcopenia include nutritional intervention, exercise intervention and drug intervention, the validity of these interventions in elderly hip fractures has not been proven clearly. Also, most studies have reported short-term results, there is no consensus on optimal long-term treatment.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






