


INTRODUCTION
Osteoporosis is a disease characterized by reduced bone mass, altered bone microarchitecture, and an increased risk of fracture, especially in elderly population.[1,2] Osteoporosis is associated with fragility fractures, which results in decreased activity, poor quality of life, high mortality and excessive economic burden.[2,3,4,5,6] Korean population is aging and osteoporosis has been one of the highlighted health care concerns in Korea.[6]
There have been several issue and concerns on osteoporosis treatment. The diagnosis of osteoporosis and the decision for treatment rely primarily on the assessment of bone mineral density (BMD) and on the inclusion of personal risk factors.[7] Assessment of BMD is the first step to diagnose and treat osteoporosis. The confirmation of reports of BMD by physician who see patient with osteoporosis is important. The fracture-risk assessment tool (FRAX®), developed by the World Health Organization (WHO), allow physicians to predict the 10-year probability of osteoporotic fracture based on risk factors, even if BMD data are not available.[8] To evaluate patients with osteoporosis, secondary osteoporosis should be kept in mind in practice, and the evaluation of vitamin D status has been highlighted. Among the anti-osteoporosis drugs, bisphosphonate has been most commonly administered in practice. Recently, long-term use of bisphosphonate has been focused due to concerns about atypical femoral fracture and osteonecrosis of jaw.[9] Although sufficient use of calcium should be necessary to gain the full effect of anti-osteoporosis drugs, some authors have warned the concerns on utilization of calcium for cardiovascular events.[10,11]
Even if physicians' attitude is very important to treat a medical condition such as osteoporosis, there was a lack of study on physicians' attitude about these contemporary issues in Korea.
The purposes of this study were to evaluate physicians' attitude in these contemporary issues including utilization of dual energy X-ray absorptiometry (DXA) and FRAX®, evaluation of vitamin D status and secondary osteoporosis, concerns on long-term use of bisphosphonate and calcium supplements for cardiovascular events, by using e-mail survey to members of Korean Society for Bone and Mineral Research (KSBMR). In addition, we also surveyed the barriers to osteoporosis treatment in Korea. This would be helpful to decide which fields should be focused in future.
METHODS
We administered a 30-item questionnaire to all members of KSBMR, who treat patients with osteoporosis. The questionnaires were sent via email including Google survey form. The email-based survey form was returned over a four week period in August 2013. It was very user-friendly, with a simple format and clear instructions. It prevented any deviations from the response options that were predefined predefined for each question by using drop boxes and check boxes. Submission of the survey was restricted until all questions were completed, which substantially reduced unanswered questions.
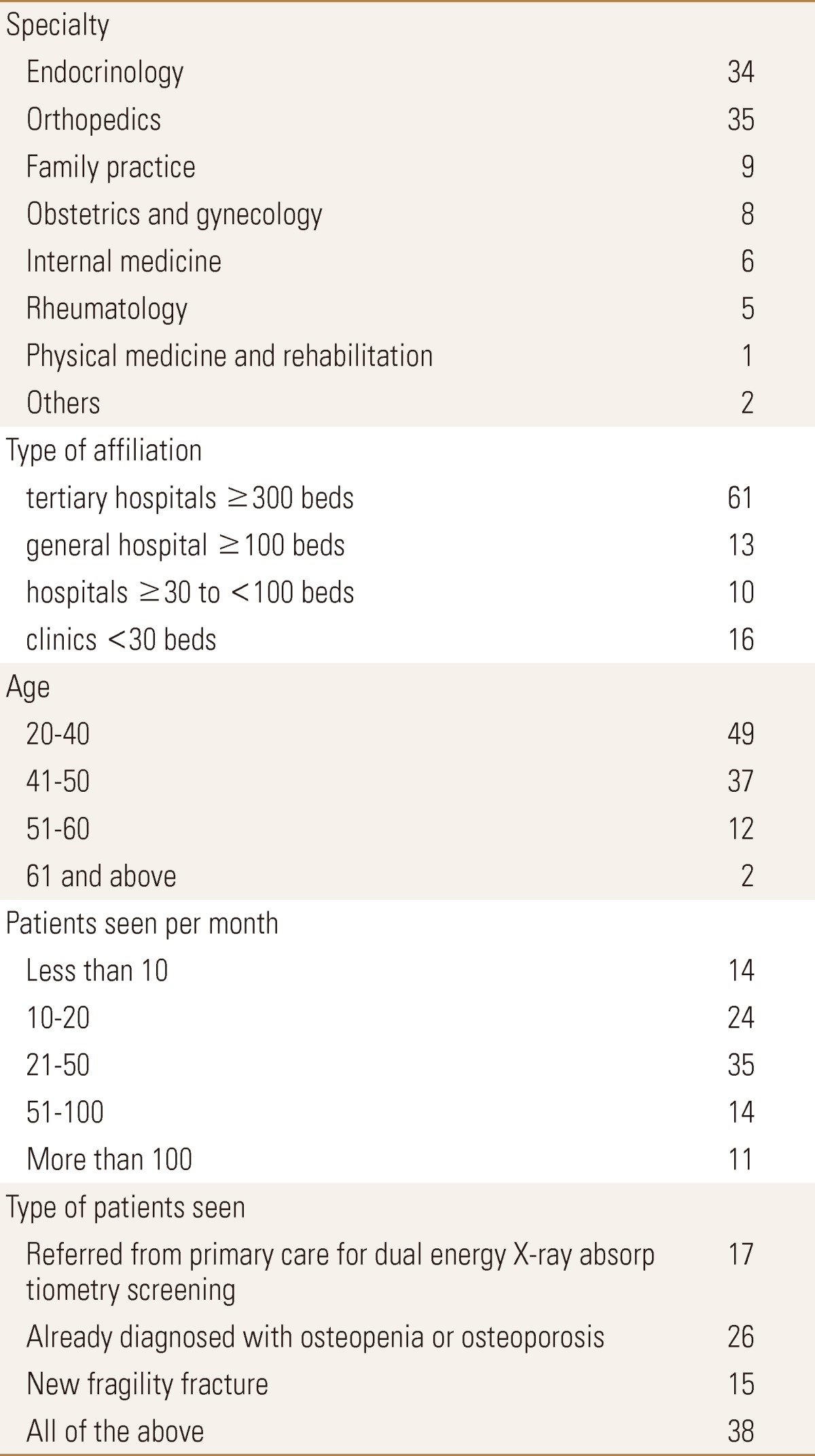
The questionnaire was composed of two parts. The first part included 6 questions which addressed demographic factors of participants. Demographic factors included background of the participants including specialty, type of affiliation according to bed size (clinics; <30 beds, hospitals; ≥30 to <100 beds, general hospitals; ≥100 beds, and tertiary hospitals; ≥300 beds), age group, the number of patients treated per month, typical type of osteoporotic patients, and type of the used densitometry (peripheral vs. central).
The second part of questionnaire consisted of 24 questions about the physicians' attitude on contemporary issue. Contemporary issue included utilization of DXA or FRAX®, evaluation of vitamin D status, evaluation for secondary osteoporosis, concerns about long-term use of bisphosphonate, and concerns about calcium for cardiovascular events. This questionnaire was made based on the questionnaires, which had been administered to participant in 2010 regional conference of the International Osteoporosis Foundation (IOF) held in Singapore.[12] After reviewing the questionnaire, we removed 4 questions and added 8 additional questions to the questionnaire. Our additional questions included concerns on calcium for cardiovascular events. Permission to conduct the survey was obtained from the organizers of the KSBMR and the questionnaire was reviewed by them prior to administration.
1. Statistical Analysis
Categorical and dichotomous variables were summarized with frequencies and percents. The Student's t-test was used to analyze continuous variables, and the Chi-square test to analyze dichotomous values. Statistically significance was accepted for a P value of <0.05, and statistical analysis was performed using SPSS statistical software (version 16; SPSS Inc., Chicago, IL, USA). This study was exempted from the institutional review board, because this study included data from the de-identified individual for public purpose.
RESULTS
Of 1,282 members of KSBMR who were asked, 104 (8.1%) returned fully completed questionnaires. The response rate for members of KSBMR was 8.1% (104 of 1,282). We exclude 4 participants who did not currently see and treat patients with osteoporosis, and analyzed remaining 100 participants. The demographical characteristics of the respondents and the characteristics of patients seen are shown in Table 1.
1. Assessment of bone mineral density
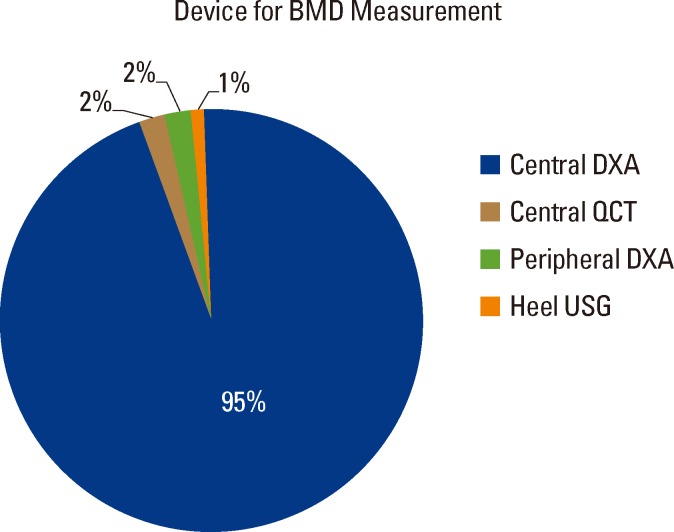
Ninety-nine percent of the respondents used bone density assessment to help them in diagnosis and making treatment decisions. The type of device that was most accessible to our respondents was central DXA (95%; Fig. 1). Seventy-eight percent of the participants indicated that they performed the reporting of bone densitometry themselves. Among the remainder, 91% (20/22) claimed that they confirmed the reporting physician's findings by looking at the scan/printout themselves.
2. Utilization of FRAX®
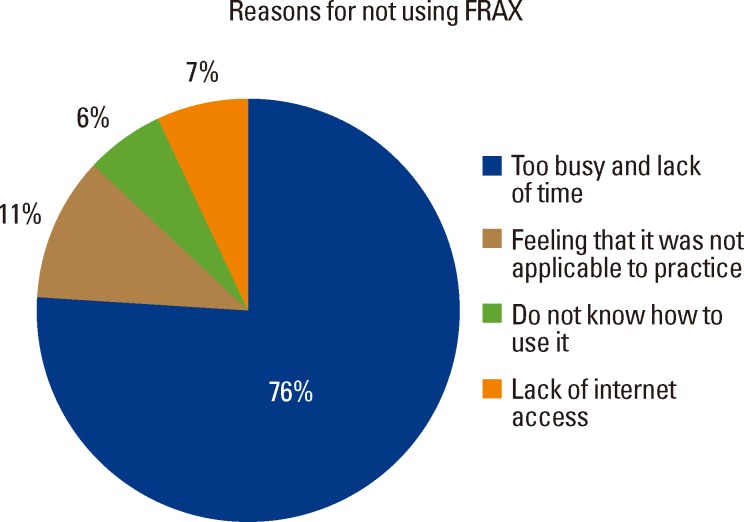
This survey showed that most respondents (88%) were aware of the FRAX® tool. About one fifth of the participants (17/88, 19.3%) who were aware of FRAX® also used it in their practice. There were no associated demographic factors with utilization of FRAX®. Among 71 responders who were aware of FRAX®, but did not use it in their practice, the primary reasons given were (a) having a practice that was too busy and hence lack of time to perform a FRAX® calculation (54/71, 76%), or (b) feeling that the FRAX® tool was not applicable to their practice (8/71, 11.3%). The remaining 12.7% (9/71) did not know how to use it or lack of internet access (Fig. 2).
3. Evaluation of vitamin D status / screening for secondary causes of osteoporosis
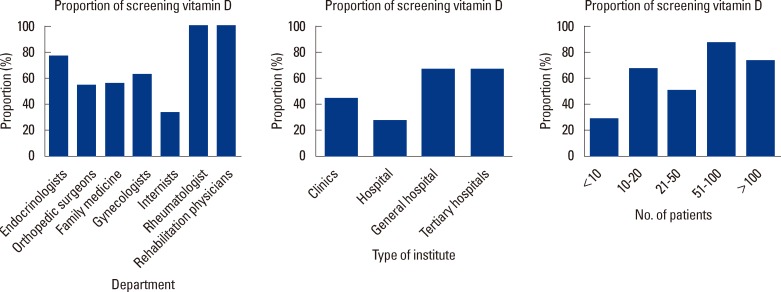
Screening for vitamin D insufficiency was performed by 59% of the respondents. In terms of subspecialty, endocrinologists were the most likely (76.5%) to screen all patients with osteoporosis and fragility fracture for vitamin D deficiency (Fig. 3). In terms of bed size, physicians in tertiary hospitals and general hospital were more likely to screen vitamin D deficiency than those in hospital and clinics. (P=0.044) (Fig. 3) Those who saw more patients with osteoporosis per month were more likely to screen all their patients for vitamin D deficiency than those who saw less (P=0.009) (Fig. 3).
Fifty-two percent of the respondents indicated that they routinely obtained blood tests to screen for secondary causes of osteoporosis before initiation of treatment with antiosteoporosis agents. In terms of subspecialty, endocrinologists were the most likely (70.6%) to obtain blood tests for secondary causes of osteoporosis. Among 48 responders, who did not perform blood test in their practice, the primary reasons given were (a) cost (35%), (b) the test was irrelevant (19%), (c) patient's refusal (17%), and (d) difficulties in interpreting the test (13%). The remaining 17% indicated lack of time or no facilities.
4. Concerns on long-term use of bisphosphonate
Almost all respondents (99%) indicated that they were aware of the recent developments concerning the potential side effects of bisphosphonates. These concerns have apparently lead to a change in management practice in the majority of participants (83/99, 83.8%), including (a) a reevaluation for the need for continued use of bisphosphonates after 5 years (61%), (b) a change of medication after 5 years (23%), (c) a change to an alternate medication (15%), as well as (d) a complete stoppage of the practice of prescribing bisphosphonates (1%).
5. Concerns on calcium for cardiovascular events
Almost all respondents (92%) indicated that they were aware of the recent developments concerning the potential side effects of bisphosphonates. These concerns have apparently lead to a change in management practice in a half of participants (50%, 46/92), including (a) decrease dose of calcium (58%), (b) decrease dose and frequency of calcium (28%), (c) decrease frequency of calcium (9%), and (d) complete stoppage of the practice of prescribing calcium (5%).
DISCUSSION
In this study, we evaluated physicians' attitude in several contemporary issues on osteoporosis treatment and identified the barriers to osteoporosis treatment in Korea, by using e-mail survey system.
First, the assessment of BMD is an important and initial step for the diagnosis and management osteoporosis, because BMD has been shown to correlate well with fracture risk.[10] In Korea, the annual check of BMD has been included in the reimbursement guidelines, and the cutoff value for reimbursement has been changed to be T-score of -2.5 since October 2011.[13] In our survey, 99% of physicians indicated that they assessed BMD in their patients, and majority of them used central DXA. International Society for Clinical Densitometry (ISCD) has recommended that Certified Clinical Densitometrist (CCD), who meet specified knowledge requirements measured through a standardized testing process.[14] However, there was no reimbursement or certification for CCD in Korea. Therefore, physicians have to confirm by themselves, although other physician could report the results of DXA. This situation was also confirmed by our survey.
Second, the FRAX® is a computer-based tool (http://www.shef.ac.uk/FRAX) for estimation of risk of osteoporotic fracture.[8] FRAX® has been available for Korean population since 2009, and most of the physicians surveyed were aware of FRAX®. However, only one fifth physicians used FRAX in their practice. Our survey showed that a significant amount of time to perform the FRAX® estimation limit its use in Korea.
Thirds, significant vitamin D deficiency might be associated with osteoporosis, because it leads to secondary hyperparathyroidism and increased bone turnover.[15,16,17] The prevalence of vitamin D inadequacy has been shown to be as high as 92% in postmenopausal women in Korea.[18,19] In our survey, universal screening for vitamin D deficiency seems not to be in the majority of practice in Korea. Vitamin D supplementation is safe and cheap for patients with osteoporotic fractures, and is recommended, if vitamin D deficiency is present, by several international guidelines.[20,21,22]
A similar scenario could be found in terms of ordering metabolic laboratory tests for other secondary causes of osteoporosis. The cost was indicated as main reason by the survey respondents who did not routinely screen for secondary osteoporosis. Although the prevalence of secondary osteoporosis was not known in Korea, the evaluation for secondary osteoporosis may lead physicians to get an opportunity to find an easily treatable cause for secondary osteoporosis.
Fourth, recently, concerns of associations between long-term use of bisphosphonate and osteonecrosis of the jaw, as well as atypical femoral fractures have been raised.[9,23,24,25] The almost respondents in our survey were aware of these new concerns and admitted to having made changes in their real practice. More than half reevaluated the need for continued use of bisphosphonates after 5 years. Although our survey did not include the question about the optimal length of treatment with bisphosphonates, literatures have shown that short to mid-term effects on bone health are satisfactory, but long-term use of bisphosphonate without drug holiday should be reevaluated in terms of risk and benefit.[9,23,24,25,26,27,28]
Fifth, several guideline for osteoporosis management include calcium supplementation, because the full effect of anti-osteoporosis drugs depends on the sufficient use of calcium.[29] In fact, compliant use calcium was associated with reduced risk of osteoporotic fracture.[30] Recently, concerns of associations between calcium supplements and cardiovascular events have been raised.[10,11] Our survey revealed that a half of participants changed their pattern of prescription for calcium.
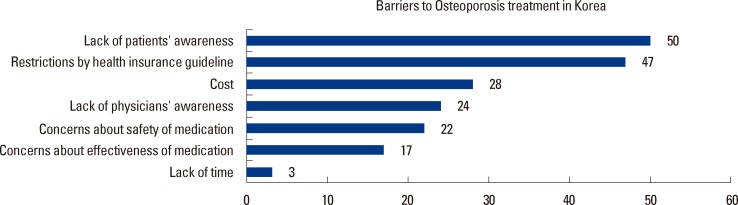
Sixth, our survey identified physicians' perceptions about barriers to osteoporosis management in Korea. A previous study reported that cost of treatment was the biggest barrier in the USA and Asia-Pacific region.[12,31] However, our survey showed that lack of patients' awareness was considered as the biggest barrier by Korean physicians. Interestingly, the restriction by health insurance guideline was the next biggest barrier identified by the survey respondents. The third biggest barrier indicated by the respondents was cost. These findings indicate the need for educational programs for patients, and the improvement of reimbursement system.
There were limitations in this study. First, there might be a selection bias, because the respondents were members of KSBMR, which means that they were actively interested in osteoporosis management. Second, only a small number of (104/1,282 members, 8.1%) physicians returned fully completed questionnaires). The results might be biased because only physicians with interest in osteoporosis may have returned the answer. Actually, 99% of the respondents assessed BMD and most of them used central DXA.
Despite a limitation, this is the first study presenting current osteoporosis management practices among physicians representing different specialties in Korea, and provides an interesting insight into the current issue for diagnostic and treatment of osteoporosis in Korea. This is also the first time that the utilization of FRAX® has been evaluated in Korea.
Our survey reveals that screening for vitamin D deficiency as well as for other secondary cause of osteoporosis is insufficiently performed in Korea. Awareness of FRAX® is present among physicians; however, majority of them does not use it-the main reason cited being the lack of time. Current concerns of long-term use of bisphosphonate and calcium supplement lead to change the physicians' practice. Important barriers to osteoporosis care are a lack of osteoporosis awareness among patients as well as costs of treatment in Korea.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






