


INTRODUCTION
Thyroid cancer is one of the most common endocrine malignancy.[1] Majority of thyroid cancer is differentiated thyroid cancer (DTC) raised from thyroid follicular epithelial cells, which are considered well-differentiated tumors, and have an overall excellent prognosis, with reported 10-year survival rates reaching 90%.[1,2,3] The excellent prognosis of DTC is because of a combination of the favorable biologic behavior of tumor cell and effective therapeutic modalities. The ‘standard’ treatment strategy for DTC includes surgery (near total/total thyroidectomy) followed by radioactive iodine (131-I) ablation of the surgical remnant and metastatic lesion, and long-term thyrotropin (TSH) suppression therapy.[3,4] DTC expresses thyroid-stimulating hormone (TSH) receptor on the cell membrane and TSH stimulates cell growth rate.[5] Thus the long-term suppression of TSH by supra-physiologic doses of L-thyroxine is used to treat patients with DTC with the purpose of decreasing the risk of cancer recurrence.[6,7,8,9,10]
However, it has been suggested that the long-term TSH suppression may be associated with potential undesired adverse effects of thyroxine on bone metabolism [11,12] as well as the major cardiovascular events [13,14,15,16,17,18] and atrial fibrillation,[19,20] because this represents in effect a state of chronic subclinical hyperthyroidism. Although normal euthyroid status during childhood and adolescence is required for acquisition of peak bone mass, overt hyperthyroidism is associated with an increased risk for osteoporosis.[21,22,23] The elevated level of thyroid hormone can excessively stimulate a bone turnover,[24] and shorten the bone remodeling cycle [25] which lead to consequent bone loss and decrease of bone mineral density (BMD). Therefore, patients who underwent TSH suppression therapy after thyroidectomy could be vulnerable to osteoporosis and decreased BMD.[19,26,27,28]
However, there is no consensus about the influence of long-term TSH suppression following thyroidectomy on BMD in patients with DTC, because of different study design (cross-sectional and longitudinal study), included patient groups (premenopausal and postmenopausal women, and men), methodology measuring BMD, area of interest for BMD (femoral neck and lumbar spine), and choice of outcome parameters (T-score, Z-score, and absolute value of BMD).[29,30,31,32]
Therefore, the purpose of this study was to determine whether TSH suppression therapy in patients with DTC influence BMD from the literature review and meta-analysis.
METHODS
This study was exempted from Institutional Review Board review because it did not involve any human subjects.
1. Search strategy
This meta-analysis was conducted according to the updated Preferred Reporting Items for Systematic review and Meta-Analysis Protocols (PRISMA-P) guidelines.[33] Searches of PubMed-Medline, EMBASE, and Cochrane Library were conducted by using key terms (“thyroid cancer or thyroidectomy” and “osteoporosis or osteoporotic fracture”) (Supplementary Appendix 1). The last search was conducted on September 26, 2018. Two authors (YJL and YKL) independently screened the titles and abstracts to identify studies on BMD in thyroid cancer. They also checked the reference lists of all potentially eligible studies and review papers to find out additional relevant publications.
2. Selection criteria
Studies were screened and selected by all investigators on the basis of a priori criteria.
The inclusion criteria were (1) published as an original article in English; (2) included TSH suppression therapy in patients with DTC; (3) controlled cross-sectional studies (patients compared to a normal control group more or less carefully matched for age, sex, and menopausal status at least); (4) evaluated the BMD as primary outcome by using dual energy X-ray absorptiometry (DXA) in femoral neck, total hip or lumbar spine; and (5) available numerical data for both patients and controls (number of patients, mean and standard deviation of BMD according to the menopausal status).
Exclusion criteria were (1) cannot evaluate numerical data for patients with DTC; if the study included other conditions such as medullary cancer and toxic goiter; (2) not included TSH suppression therapy; (3) not available menopausal status; (4) measured BMD not by using DXA; (5) not reported value of BMD of femoral neck, total hip or lumbar spine; (6) not have normal control group; and (7) reviews and collection of abstracts for conference meeting.
Two authors (YJL and YKL) reviewed the retrieved full manuscripts to determine whether value of BMD after TSH suppression therapy in patients with DTC in femoral neck or lumbar spine had been reported.
3. Outcome measure and data extraction
The primary outcomes for the meta-analysis was the difference of BMD between patients with TSH suppression therapy after surgery for DTC and control group.
The studies were categorized according to gender and menopausal state and subgroup analysis undertaken accordingly (premenopausal women, postmenopausal women, and men).
For every eligible study, the following data were extracted and entered in a spread sheet by the 2 reviewers: the family name of the first author, year of publication, country, number of patients, mean duration of TSH suppression therapy, sample characteristics (age and gender), the mean value of BMD (g/cm2) in femoral neck or lumbar spine.
4. Quality assessment and publication bias
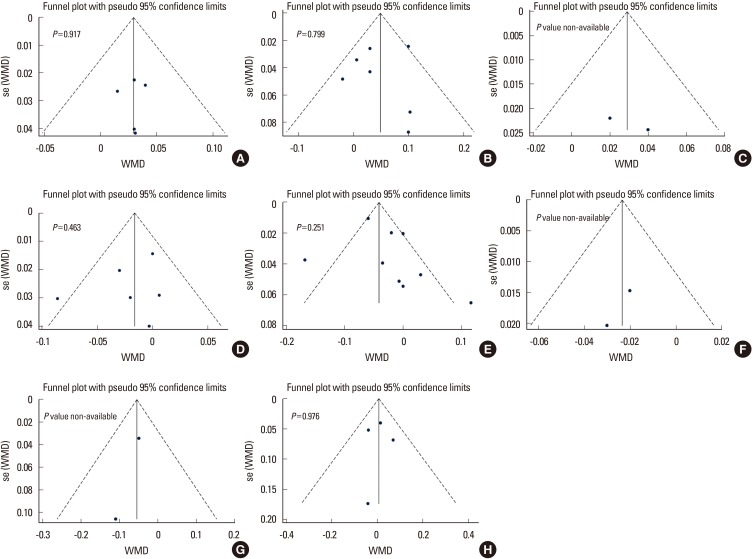
Two of the authors (YJL and YKL) independently evaluated the quality of all the studies, using Newcastle-Ottawa Scales.[34] This tool comprises three parameters: selection, comparability, and outcome. Each parameter consists of subcategorized questions: selection (a maximum of 4 stars), comparability (a maximum of 2 stars), and exposure or outcome (a maximum of 3 stars). We assessed the publication bias with Begg's funnel plot [35] and Egger's test [36].
5. Statistical analysis
We calculated the weighted mean difference (WMD) representing the magnitude of the difference between the comparative groups for each outcome, because all studies used the same outcome and unit of measurement (g/cm2).[37] WMD were computed separately for all available treatment and control groups for each study. We had used a fixed-effects or random-effects model depending on the results of heterogeneity to quantify the pooled effect size of the included studies (Values of P-value of less than 0.1 or an I2 value higher than 50% meant significant heterogeneity and a random-effects model should be applied). All analyses were performed using STATA (version 14.0; Stata Corp., College Station, TX, USA).
RESULTS
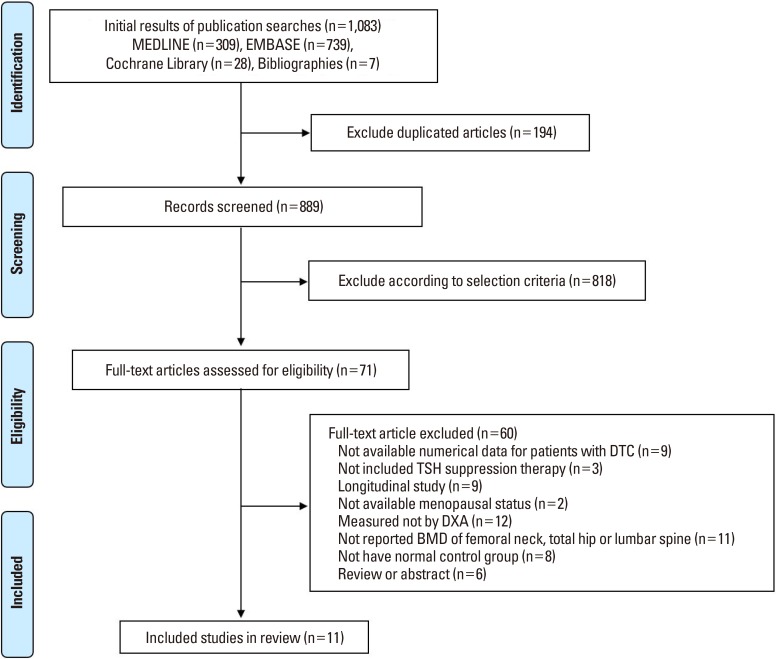
A primary search from the PubMed-Medline, EMBASE, and Cochrane Library, yielded 1,083 published articles. After duplicates removed, 889 articles were primarily screened by title and abstract. As a result, 71 articles were selected and reviewed for eligibility by full-text papers and a total of 11 cross-sectional studies fulfilling all inclusion criteria were included in the final analysis (Fig. 1).[11,38,39,40,41,42,43,44,45,46,47]
The results of the subgroup analyses according to gender and menopausal state were as follows.
1. Premenopausal women
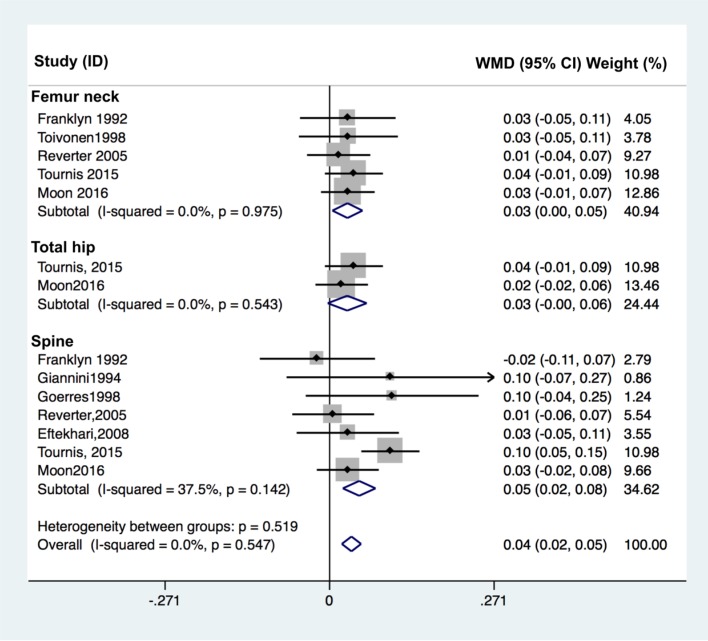
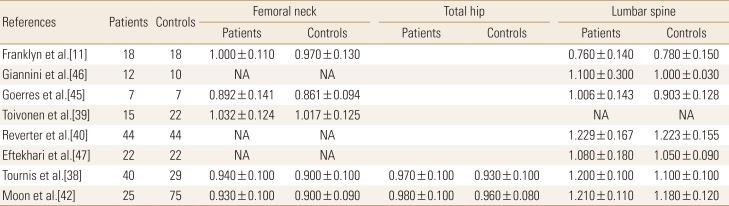
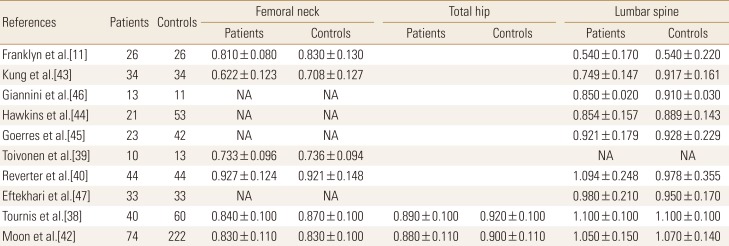
The effect of TSH suppression therapy on BMD in premenopausal women is described in 8 studies involving a total of 183 patients and 227 controls (Table 1). Femoral neck BMD (pooled WMD, 0.029; 95% confidence interval [CI], 0.005-0.054; P=0.020), and spine BMD (pooled WMD, 0.049; 95% CI, 0.022-0.076; P<0.001) were significantly higher in patients with TSH suppression therapy than control group, while total hip BMD (pooled WMD, 0.029; 95% CI, −0.003 to 0.061; P=0.076) did not differ significantly in premenopausal women (Fig. 2).
2. Postmenopausal women
The effect of TSH suppression therapy in postmenopausal women was investigated in 10 studies involving a total 318 patients and 538 controls (Table 2). Total hip BMD (pooled WMD, −0.023; 95% CI, −0.047 to 0.000; P=0.050), and spine BMD (pooled WMD, −0.041; 95% CI, −0.057 to −0.026; P<0.001) and were significantly lower in patients with TSH suppression therapy than control group, while femoral neck BMD (pooled WMD, −0.016; 95% CI −0.035 to 0.002; P=0.084) did not differ significantly (Fig. 3).
3. Men
Four studies involving a total 66 patients and 67 controls were identified for analysis addressed the effects of TSH suppression therapy on bone metabolism in men in a cross-sectional study design (Table 3). No study showed a significant difference of BMD between patients and controls. Femoral neck BMD (pooled WMD, −0.055; 95% CI, −0.119 to 0.009; P=0.094), and spine BMD (pooled WMD, 0.007; 95% CI, −0.049 to 0.063; P=0.803) did not differ significantly in men (Fig. 4).
4. Quality assessment and publication bias
In terms of the methodological quality, the mean value of the awarded star was 5.3 (5 stars [2 studies], 6 stars [9 studies]; Supplementary Table 1). The Begg's funnel plot was not asymmetrical, and P-value for bias were not significant in all outcomes (Fig. 5).
DISCUSSION
The clinical implications of long-term TSH suppression therapy on bone are critical, largely because of the favorable prognosis of DTC and long-term survival of patients with DTC.[10] Subclinical thyroid dysfunction has been known to be associated with increased risk of hip fracture,[48] but the influence of chronic subclinical hyperthyroidism, TSH suppression therapy, on decreased BMD in patients who underwent thyroidectomy for DTC remain controversial. Our aim was to review the literature on the effects of TSH suppression therapy on BMD in patients with DTC.
Although there have been many studies on this issue, each study had a different outcome as well as different tools for measurement of BMD. Many previous studies have used single or dual photon absorptiometry, not DXA.[49,50,51,52,53,54]
The majority of studies reported no effect of TSH suppression therapy on BMD in men and premenopausal women.[40,41,42] Our meta-analysis also showed no influence of TSH suppression therapy on BMD in men and premenopausal women. On the other hands, the influence in postmenopausal women remain unclear. Our meta-analysis showed the TSH suppression therapy was associated with lower BMD of total hip and spine in postmenopausal women. We could not determine conclusively this issue, because of too small number of the included studies and pooled patients, although we performed a meta-analysis.
However, some large population-based cohort studies showed the increased risk of osteoporosis and osteoporotic fracture such as hip fracture and vertebral fracture.[55,56] Lin et al.[56] compared the risk of osteoporosis and osteoporotic fracture among 9,398 thyroid cancer patients with levothyroxine use (n=538), those (n=8,860) without levothyroxine use and propensity-score-matched controls (n=9,398). They showed that the incidence of osteoporosis and osteoporotic fracture in the thyroid cancer patients (8.69/1,000 person-years) was higher than that in the non-thyroid-cancer cohort (6.60/1,000 person-years) (adjusted hazard ratio, 1.39; 95% CI, 1.22-1.58). They also presented that long duration of levothyroxine use, and high cumulative dose of levothyroxine were significantly associated with an increased risk of osteoporosis in thyroid cancer patients following thyroidectomy.[56]
Based on our meta-analysis of available data, we identified postmenopausal women with DTC receiving TSH suppression therapy as a risk group for bone loss. Considering menopause as the most important risk factor of osteoporosis,[57] the discrepancy in results between premenopausal and postmenopausal women might be explained by a different susceptibility according to menopausal status.
The present study has a limitation. The cumulative sample size was not very large because most of the studies included relatively few patients. Thus the results of subgroup analysis are also very limited due to small sample size. But we used the weighted effect sizes by including studies only had used DXA, the effect size is easily interpreted from a clinical point of view.
CONCLUSIONS
Overall, although studies were limited by small numbers, results suggested possible association between chronic TSH suppression therapy and the higher risk of low BMD in postmenopausal women with TSH suppression therapy. And, it is clear that larger-scale, better-designed studies that report effects of TSH suppression therapy on BMD are needed in the future to determine the influence of TSH suppression therapy on risk of osteoporotic fracture in DTC.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Supplement1
Supplement1 Print
Print






