Association of Serum 25-hydroxy-vitamin D Concentration and Arterial Stiffness among Korean Adults in Single Center
Article information
Abstract
Background
There are growing concerns about the role of vitamin D deficiency in cardiovascular diseases. Therefore, we investigated the correlation between serum 25-hydroxy-vitamin D (25[OH]D) and arterial stiffness among Korean adults.
Methods
We retrospectively reviewed the medical charts of 302 people (115 women and 187 men) who visited a tertiary hospital from January 2015 to December 2016. Serum 25(OH)D was measured using the radioimmunoassay technique, and brachial-ankle pulse wave velocity (baPWV) was measured using an automatic wave analyzer. We obtained the doctor's report on the medical history of the participants, their alcohol consumption and smoking habits, and their exercise status. Metabolic syndrome was diagnosed based on guidelines from the National Cholesterol Education Program (NCEP)-Adult Treatment Panel (ATP III) and the International Diabetes Federation (IDF). Results of basic blood tests and physical assessment were also collected.
Results
In the Pearson correlation analysis, serum 25(OH)D and baPWV showed a statistically significant inverse relationship (r=-0.279, P<0.001). Using multiple regression analysis, and after adjusting for possible confounders, serum 25(OH)D concentration was found to be significantly associated with baPWV (β=-0.121, P=0.011).
Conclusions
We observed an association between serum 25(OH)D concentration and arterial stiffness. Further studies involving larger sample sizes will be needed to confirm this associations.
INTRODUCTION
Vitamin D is synthesized in the body, and can be considered a hormone that has endocrine, autocrine, and paracrine functions. Vitamin D regulates calcium homeostasis and mineral metabolism by influencing the activities of the intestines, bones and kidneys. In addition, vitamin D is essential for the induction of cellular differentiation as well as for the inhibition of angiogenesis.[12] Vitamin D also has a number of nonskeletal effects that may favorably affect the cardiovascular system, for example, downregulation of the renin-angiotensin system,[3] stimulation of insulin sensitivity in pancreatic beta (β)-cells,[4] and modulation of inflammation.[5]
Presently, vitamin D deficiency is recognized as a worldwide concern,[6] and in Koreans especially, this deficiency is very common. The fourth Korean National Health and Nutrition Examination Survey (KNHANES V-1 and 2) reported a particularly high prevalence of vitamin D deficiency (25-hydroxy-vitamin D [25(OH)D] <20 ng/mL) in up to 60% of Koreans aged ≥10 years (65.9% of males and 77.7% of females).[7]
There are growing concerns about the role of vitamin D deficiency in cardiovascular diseases. Previous clinical studies have confirmed that low vitamin D levels (defined as serum 25(OH)D concentration below 20 ng/mL according to guidelines from The Endocrine Society can impair vascular function. This may compromise vascular compliance (the elastic property of blood vessels), thereby manifesting as increased arterial stiffness.[8]
Arterial stiffness is an early marker of atherosclerotic diseases. Increased arterial stiffness has been shown to be an independent risk factor for both cardiovascular disease and overall mortality in elderly patients.[9101112] Pulse wave velocity (PWV) is a simple, economical, and the most widely used non-invasive examination method for measuring arterial stiffness.[13] Several studies have investigated the association between vitamin D status and arterial stiffness using PWV. However, most of these studies were performed in Western countries,[141516171819] with only a few Asian studies.[202122] Moreover, only a few studies have involved Koreans,[2324] and a recent study has observed no significant relationship between vitamin D status and arterial stiffness. [24] Even a meta-analysis of various studies has produced the same result.[25] However, there are many studies that have shown vitamin D to have a positive effect against arterial stiffness.[2627282930] We hypothesized that a higher concentration of serum 25(OH)D leads to reduced arterial stiffness. Therefore, we evaluated the relationship between 25(OH)D concentration and brachial-ankle PWV (baPWV) in Korean adults.
METHODS
1. Study subjects
A total of 302 participants (age≥20 years) who had undergone medical checkups at a tertiary healthcare facility, between January 2015 and December 2016 were included in the study. Information about lifestyle, medical history, drug history, and alcohol consumption, smoking habits and exercise status were obtained from the doctor's notes. Body weight and height were measured in light clothing without shoes, and body mass index (BMI) was calculated as the weight divided by the height squared (kg/m2). Waist circumference (WC) was measured at the midpoint between the iliac crest and the lower rib margin. All participants had already undergone a basic regular blood examination, as well as examinations for baPWV and 25(OH)D. Blood samples were collected from all participants after at least 8 hr of fasting. Participants were made to rest for at least 5 min before the blood pressure (BP) was measured on the right arm using and electronic device.
After reviewing the health screening charts, patients with a history of dyslipidemia (n=34), cardiovascular diseases (n=8), cerebrovascular diseases (n=2), any type of cancer (n=13) were excluded from the study.
2. Study methods
Vitamin D status is commonly assessed by measuring 25(OH)D level. This is because unlike 1,25 dihydroxy-vitamin D (1,25[OH]2D), 25(OH)D has a longer half-life and its activity is not affected by the parathyroid hormone.[31] Blood samples were analyzed and 25(OH)D measured, using a radioimmunoassay (ADVIA Centaur XPT Immunoassay System; Siemens, Erlangen, Germany). The lowest measurable concentration of 25(OH)D was 4.2 ng/mL. Vitamin D deficiency was defined as a serum concentration of 25(OH)D, <20 ng/mL, while vitamin D insufficiency was defined as a serum concentration of 25(OH)D ≥20 ng/mL, but <30 ng/mL.[3233]
Participants were made to rest for 5 min in the supine position before PWV was measured using an automatic waveform analyzer (VP-1000 plus; Omron Co., Ltd., Kyoto, Japan). The PWV between the brachial arteries and the ankle was measured by placing both arms and the ankle in a cuff, to which an oscillometric sensor was implanted. In this study, the average value of both the right and left baPWV was calculated and used in the analyses.[34]
Regular alcohol drinkers were defined as those whose records showed a consumption of more than one bottle per week, while all other participants were defined as non-drinkers. Smokers were defined as those who had smoked more than five packs of cigarettes during their lifetimes and were smoking currently. The remaining participants were defined as nonsmokers. Regular exercise was defined as performing exercise for more than 3 days in a week for 30 min per session.
Information about any previous diagnoses of hypertension (HTN) and diabetes mellitus (DM) were obtained through health interviews. Guidelines from the National Cholesterol Education Program (NCEP)-Adult Treatment Panel (ATP III) and the International Diabetes Federation (IDF) were employed in diagnosing metabolic syndrome.
The presence of metabolic syndrome was defined as when a participants met ≥3 of any of the following diagnostic criteria. 1) WC ≥90 cm (male), ≥85 cm (female), 2) triglycerides (TG) ≥150 mg/dL, 3) high-density lipoprotein cholesterol (HDL-C) ≤40 mg/dL (male), ≤50 mg/dL (female), 4) BP ≥130/85 mmHg or previously diagnosed HTN, 5) fasting blood glucose (FBG) ≥110 mg/dL or previously diagnosed type 2 DM.
3. Statistical analysis
Statistical analyses were performed using the SPSS version 12.0 (SPSS Inc., Chicago, IL, USA), and the variables are presented as mean±standard deviation. Results were computed as two-tailed, and the level of statistical significance was set at P<0.05. We compared baseline characteristics between the male and female participants using the chi-square test and independent t-test. The difference in PWV was analyzed according to history of HTN, DM, presence of metabolic syndrome, smoking, alcohol consumption, and exercise habit with the independent t-test; the Pearson correlation coefficients were used to assess the relationships among biochemical factors, clinical factors, and PWV.
Using independent t-test and Pearson correlation analysis, a multiple regression analysis was conducted on statistically significant variables as covariates and PWV as the dependent variable. Some variables (alcohol consumption, smoking, exercise) that were not statistically significant (P>0.05), but could be confounding factors were also included as covariates. In the multiple regression analysis that included systolic BP (sBP), diastolic BP (dBP), and FBG as covariates, although a history of HTN and DM were statistically significant factors according to the independent t-test, they were excluded in the multiple regression analysis owing to multicollinearity.
RESULTS
The baseline characteristics of the patients are reported in Table 1. A total of 302 participants were included in the study. This consisted of 115 women and 187 men with mean age of 55.6 years and 54.7 years, respectively. The differences in BMI, WC, dBP, low-density lipoprotein cholesterol (LDL-C), TG, HDL-C, FBG, alcohol consumption status, and smoking status were statistically different between men and women.
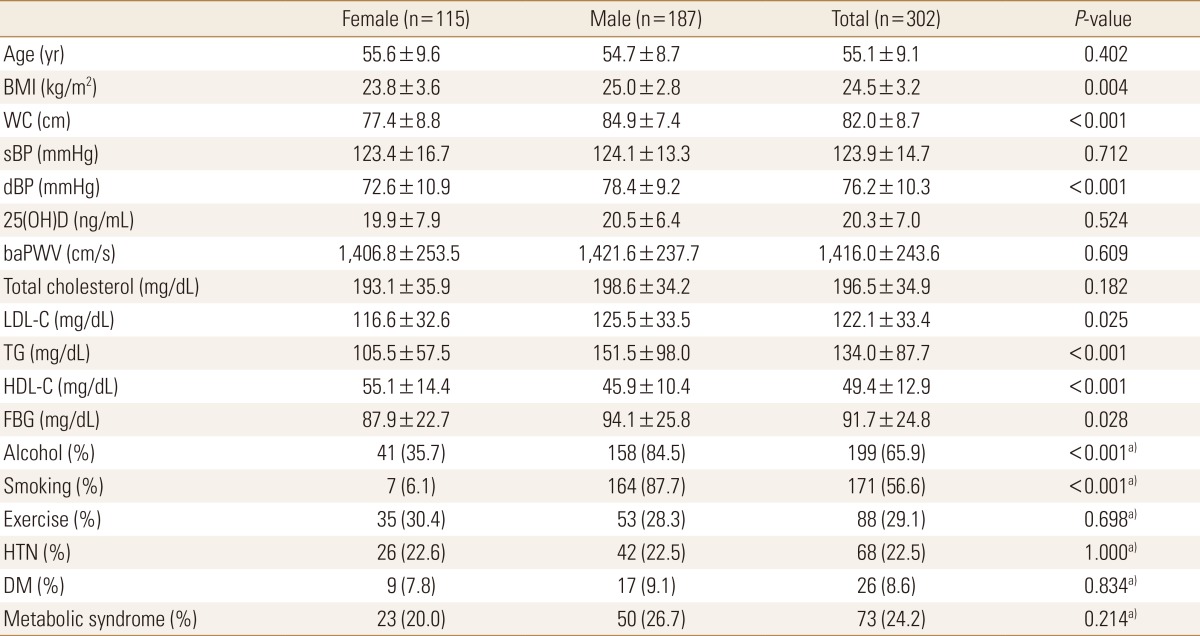
Baseline characteristics of the patients
Mean serum concentration of 25(OH)D was lower in women (19.9 ng/mL) than in men (20.5 ng/mL), although the difference was statistically insignificant (P=0.524). However, the prevalence of vitamin D deficiency (i.e. 25(OH)D <20 ng/mL) was significantly higher in women than in men (55.7% and 42.2% respectively, P=0.025) (Data is not shown).
Mean baPWV was higher in men, although the difference was not significant. (1,406.8 cm/s vs. 1,421.6 cm/s, P=0.609) (Table 1). An independent t-test conducted to analyze the relationship between baPWV and various underlying conditions yielded statistically significant differences for HTN (1,557.7 cm/s vs. 1,374.8 cm/s, P<0.001), DM (1,521.9 cm/s vs. 1,406.0 cm/s, P=0.020) and presence of metabolic syndrome (1,540.5 cm/s vs. 1,376.3 cm/s, P<0.001) (Table 2).
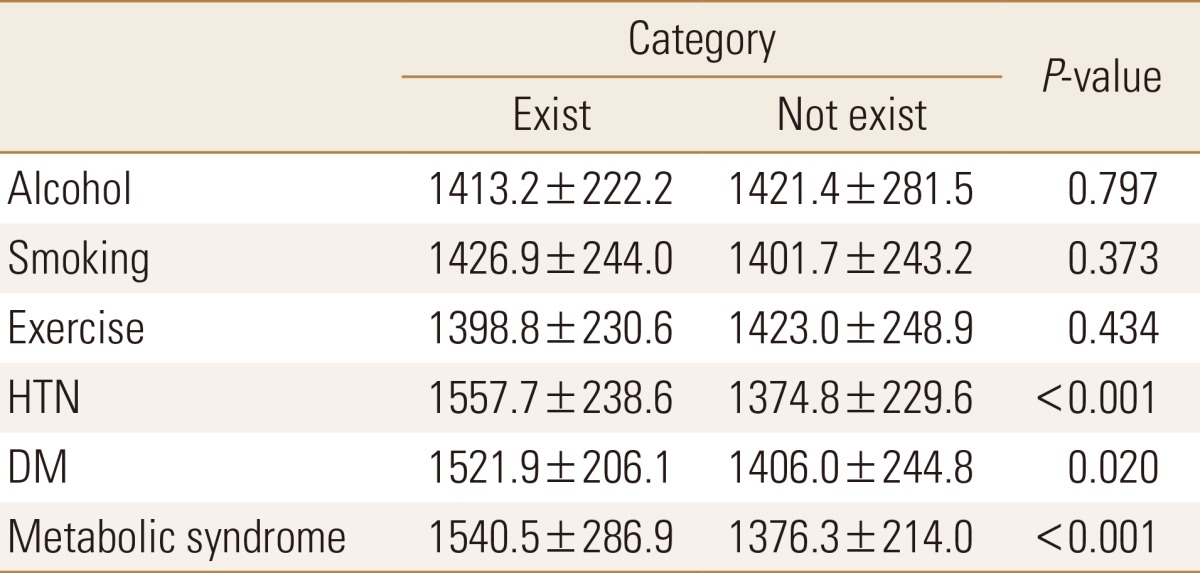
Independent t-test between brachial-ankle pulse wave velocity and multiple confounders
Univariate relationships between baPWV and parameters are shown in Table 3. baPWV positively correlated with age, WC, sBP, dBP, TG, and FBG and baPWV negatively correlated with 25(OH)D (r=-0.279, P<0.001) and HDL-C.

Pearson's correlation coefficients between brachial-ankle pulse wave velocity and parameters
In a fully adjusted multiple regression analysis, age, sBP, FBG, WC, and 25(OH)D (β=-0.121, P=0.011) were independently associated with baPWV, whereas sex, BMI, dBP, alcohol consumption, smoking, exercise status, presence of metabolic syndrome, and all lipid profiles (total cholesterol, LDL-C, TG, and HDL-C) were not. This regression model accounted for 51.7% (R2=0.517) of the total variance of baPWV (Table 4). The Durbin-Watson coefficient was 1.911, the fit test for multiple linear regression model was suitable (F=19.049, P<0.001) and all variance inflation factors of independent variables were under 10. The results of the correlation between 25(OH)D and baPWV, are represented in a scatter diagram (Fig. 1).
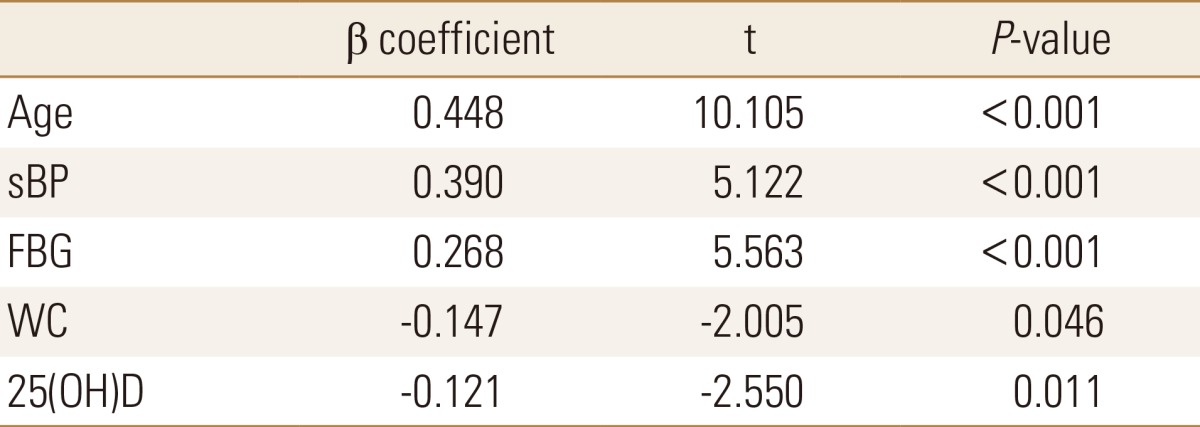
Multiple regression analysis for brachial-ankle pulse wave velocity
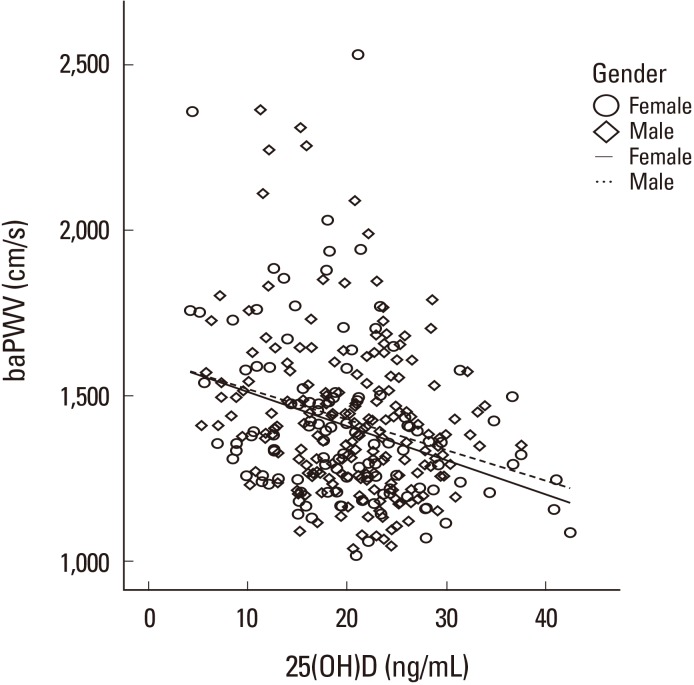
Correlation between 25-hydroxy-vitamin D (25[OH]D) and brachial-ankle pulse wave velocity (baPWV), scatter diagram.
DISCUSSION
Our study demonstrated that arterial stiffness is significantly associated with low serum concentration of 25(OH)D. The Korean Vascular Research Working Group (KVRWG) suggested age and BP as major factors that influence arterial function. The present study, however, demonstrated a statistically significant relationship between 25(OH)D and arterial stiffness even after adjustment for age and BP. In addition, we found relatively higher mean serum concentrations of 25(OH)D in participants (19.9 ng/mL in women, 20.5 ng/mL in men, aged 29-84 years) from this study than in other Korean adults (aged 20-87 years) from KNHANES database between 2008 and 2010. (16.9 ng/mL in women, 19.5 ng/mL in men).[24] We also found arterial stiffness to statistically correlate with FBG and WC.
The effects of vitamin D on the cardiovascular system are very important. Vitamin D receptors are found in many cells of the cardiovascular system.[31] Several adequate mechanisms explain how vitamin D may influence the cardiovascular system. An in vitro study has demonstrated that adequate vitamin D is associated with increased vascular endothelial cell (EC) expression of nuclear factor-kappa beta and interleukin-6, two important inflammatory mediators.[35] Moreover, vitamin D may attenuate the adverse effects of advanced glycation end products on EC expression, which would have otherwise provoked dysfunction.[36] Another study suggested that exogenous supplementation of vitamin D resulted in decreased EC proliferation and that EC stress upregulates vitamin D receptor expression on EC creating an autocrine or paracrine role for vitamin D with the potential to modulate EC adhesion and vascular smooth muscle cell migration and proliferation.[37] These results only confirm that vitamin D is important for proper functioning of the cardiovascular system.
Although several previous studies have presented inconsistent finding,[15383940] two other cross-sectional studies observed an inverse relationship between serum 25(OH)D level and arterial stiffness.[1532] In the Framingham offspring study as well, vitamin D deficiency was found to be associated with an increased incidence of cardiovascular diseases.[41] Several studies have observed a successful decrease in baPWV prior to supplementation with vitamin D.[2627282930] However, a European cross-sectional study [40] as well as a cross-sectional analysis of the Korean Longitudinal Study on Health and Aging (KLoSHA) [39] showed no association between serum concentration of 25(OH)D and baPWV.
A recent cross-sectional study among Korean adults confirmed that the positive association between 25(OH)D and baPWV was reversed when BP was controlled.[24] As mentioned earlier, BP plays a major role in influencing arterial function. Arterial stiffness results from structural and functional changes to the vascular tree,[34] and high BP may affect those changes.[42] One study among Koreans demonstrated that a statistically significant association between 25(OH)D and baPWV was only existent in patients with type 2 DM.[23] They concluded that such a relationship between 25(OH)D and type 2 DM is believed to be caused by insulin resistance and impaired β-cell function among vitamin D deficient patients.[434445]
Many studies have had inconsistent result in this area until quite recently, our study has a few strengths. To the best of our knowledge, our study may represent the first evidence of significant linear association between serum 25(OH)D concentration and arterial stiffness among Korean adults. Our study also included data on sBP, dBP, FBG, history of HTN and history of DM as possible confounding variables. Through multiple linear regression analysis, we demonstrated that sBP and FBG significantly correlated with baPWV. Nonetheless, we found serum 25(OH)D concentration to be an independent risk factor of arterial stiffness (β=-0.121, P=0.011). These results are in contrast with those observed in most recent cross-sectional studies among Korean adults,[24] although their study was conducted with a rural population, whereas our study was conducted with an urban population. Also, in our study, we obtained information from the screening medical chart of those who went for health medical examinations at the healthcare facility. Thus these individuals are more concerned about their health. In addition, there may be some differences in terms of physical activity, sun exposure, their sunscreen use, and eating habits.
Most of the vitamin D in the body is synthesized in the skin, through absorption of ultraviolet rays. Owing to the decreasing amount of time spent outdoors, the number of vitamin D deficient people is increasing. A study conducted in obese older adults demonstrated that physical activity may be required to enhance the effect of vitamin D.[46] Therefore, it is important to spend more time outdoors and increase physical activity level.
Our study has a few limitations. Firstly, the study was performed on individuals only in a single center in Korea, with a sample size of only 302 participants. Therefore, the findings may not be representative of the total adult population in Korea. Second, this was a cross-sectional study that employed assessment of screening charts, thereby rendering it difficult to determine causal relationships. Additionally, data collection errors may have occurred, as information regarding tobacco and alcohol use, exercise status, and medical history were obtained from the doctor's consultation notes and may not be a true reflection of the actual situation. Furthermore, we used single measurements of serum 25(OH)D concentration as indicators of vitamin D status; thus this may not accurately reflect long-term vitamin D status. Lastly, we did not consider other factors that could directly affect vitamin D status such as seasonal variation, duration of sun exposure, sunscreen use, skin pigmentation, vitamin D supplementation or medication, eating habits, and parathyroid hormone level.
In conclusion, an adequate serum concentration of 25(OH)D has a beneficial effect on arterial stiffness after adjusting for cardiometabolic factors. However, owing to certain limitations such as small sample size and confounders such as seasonal variations and the unknown parathyroid hormone levels, larger prospective studies are necessary to confirm these associations.
Notes
No potential conflict of interest relevant to this article was reported.