


INTRODUCTION
Osteoporosis is a systemic skeletal disease characterized by low bone mass and micro-architectural deterioration of bone tissue, with a consequent increase in bone fragility and susceptibility to fracture.[1,2,3,4]
Bisphosphonate is the most widely used drugs to prevent and treat osteoporosis.[5,6,7,8,9] Although bisphosphonate is effective for the treatment of osteoporosis and prevention of osteoporotic fractures, poor medication compliance is a key-limiting factor in terms of the prevention and treatment of osteoporosis.[5,6,7,10,11] Bisphosphonate-related factors including gastroesophaseal irritation and complex method of ingestion have been well-known risk factors for low compliance with bisphosphonate.[12,13,14] To overcome poor compliance, new type of bisphosphonate with various dose intervals have introduced. Bisphosphonates with longer interval have shown better compliance.[15,16,17]
However, there have been few intervention studies on improving compliance with bisphosphonate. Our purpose was to determine whether alarm clock could improve compliance with weekly bisphosphonate in patients with osteoporosis, by comparing with age- and gender-matched control group without alarm clock.
METHODS
This is a case-control study conducted with prospectively complied data.
From May 2012 to May 2013, 50 patients with osteoporosis were recruited and participated in alarm clock group. The inclusion criteria were (1) 65 years of age and over, (2) diagnosis of osteoporosis (T-score below -2.5 standard deviation) based on the most recent bone mineral density (BMD) measurements (hip or spine, dual energy X-ray absorptiometry [DXA]), (3) without contraindications to oral bisphosphonate, (4) no cognitive impairment, and (4) ability of interview independently. All eligibility patients were asked to take orally weekly risedronate for 1 year, and received alarm clock to inform the time of taking oral bisphosphonate weekly (Fig. 1). Clocks were provided by Sanofi Aventis. In order to avoid selection bias, written informed consent was not required.
To obtain control group, the propensity score matching with age and gender was used. As control group, 50 patients, who had taken weekly oral risedronate for treatment of osteoporosis and were followed up for 12 months or more, were identified from patients with osteoporosis medication between 2005 and 2010. The medical records whom they had not received alarm clock in were reviewed to evaluate compliance with bisphosphonate.
To compare the compliance between two groups, we analyzed compliance with bisphosphonates during 12 months after first prescription. Compliance with bisphosphonates was measured a period of 1 year of treatment after first prescription by using medication possession ratio (MPR) as the parameter.[9,18] MPR was defined as the sum of days of supply of osteoporosis medications divided by the length of follow-up, i.e., 365 days. Compliance was categorized with MPR<80% and MPR≥80%.[18,19]
The study protocol was reviewed and approved by the Institutional Review Boards and Ethics Committee.
RESULTS
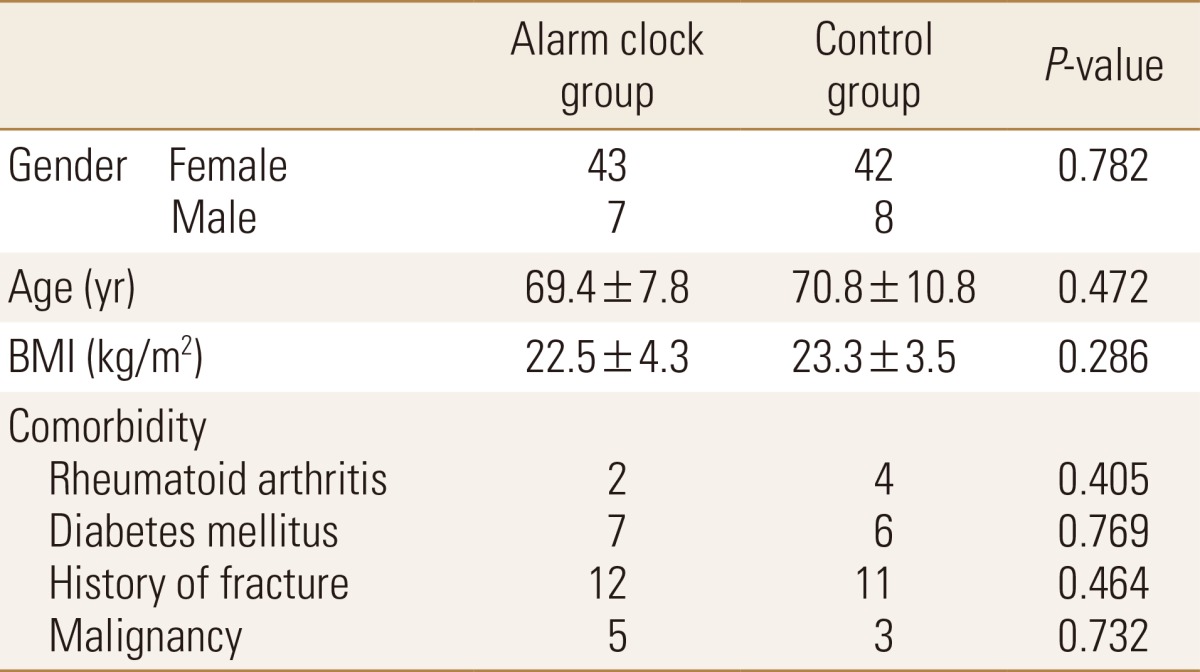
There was no significant difference of baseline characteristics including age and gender between both groups (Table 1).
The mean MPR (0.80±0.33) of alarm clock group was higher than that (0.56±0.34) of control group (P<0.001).
DISCUSSION
To our knowledge, this is the first study that evaluates compliance with weekly oral bisphosphonate in patients alarmed with clock. This study presented that alarming could improve the compliance with weekly bisphosphonate in patients with osteoporosis.
Poor compliance is a major challenge in contemporary therapeutics, because osteoporosis has asymptomatic feature itself like other silent chronic diseases. Higher ages, low socioeconomic status, low awareness on osteoporosis, various interval of administration, and adverse effect of bisphosphonate have been presented to be risk factors for low compliance with bisphosphonate.[12,13,14] Identifying patients with high risk of low compliance and efforts to increase compliance are very important in treatment of osteoporosis.
Complex dosing schedules related to other chronic diseases, such as hypertension, hyperlipidemia, and diabetes mellitus could lead to lack of compliance for osteoporosis medication. Simply forgetting to take the medication may also result in non-persistence or non-compliance in old ages.[20,21] In a previous study, 24% of the patients answered that they occasionally forgot to refill a prescription, as the reason why they did not fill prescriptions with drug regimens.[21] Therefore, it is important to alarm patients taking the medication, not to forget.
In this study, the MPR (0.56) of oral bisphosphonate without alarm clock is similar with that of another study.[22,23] However, weekly bisphosphonate with alarm clock could improve MPR (0.80) obviously in this study.
In this study, we used clock with alarming function. Currently, this intervention using alarming can be conducted with smartphone or message service using IT technology.
There are some limitations. First, we did not perform randomized study, but used historical control group. But, not to intervene control group will be ethical problem. Second, we included only patients with weekly oral bisphosphonate. Third, we did not evaluate the change of BMD and compare the incidence of osteoporotic fracture. Fourth, we did not calculate a sample size prior to study. But, power of this study was 94.5% with type 1 error of 5%.
This study, which is the first study to intervene for compliance with bisphosphonate, presented that alarming could improve the compliance with weekly bisphosphonate in patients with osteoporosis.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






