


INTRODUCTION
Osteoporosis is the most common disease of human bone, and about 33.3% of females are receiving medical treatment related to osteoporosis.[1,2] Elderly patients with osteoporosis have a greater risk of vertebrae, hip, and wrist fractures.[3] Vertebral compression fracture is the most common fracture related to osteoporosis.[4] According to a report in 2012, the standardized prevalence of vertebral fractures in Korea is 8.8% in men and 12.6% in women.[5] The prevalence of osteoporotic vertebral compression fracture (OVCF) is reported at about 40% in the elderly.[6]
OVCF is associated with several morbidities, such as chronic disabling pain, limited physical activity, progressive kyphosis, loss of functional capabilities, and decreased recreational activities.[7,8] There have been many reports of decreased quality of life (QOL) with OVCF, even in healed patients.[4,6,9,10,11,12,13,14] In addition, mortality risk is higher in OVCF patients than in patients without fracture.[15]
Generally, problems related to OVCF are self-limiting with benign features. For example, pain after acute vertebral fracture was regarded as significant for up to 6 weeks, and chronic pain was maintained only in patients with multiple compression fractures, height loss, and low bone density.[16] Some authors have reported that pain decreased by approximately 40% at day 30, and acute fracture pain decreased by 33% at day 14.[17,18] There are differing opinions that worsening health can last for many years and have sequelae.[19,20,21,22,23] A recent meta-analysis reported that QOL was reduced in OVCF patients in a way that was not fully explained by pain.[24] A previous study of patients who had OVCF an average of 5.1 years reported significantly worse QOL than control subjects.[19] However, there are few studies on patients with healed fractures.
Due to its high prevalence and significant effects on patients, QOL in OVCF is important. Quality-adjusted life-year (QALY) is a measurement used in cost-utility analysis that should be calibrated using social preference weights that reflect the general population.[25] There are several tools used to measure health-related QOL (HRQOL), such as short form-36 (SF-36) and the health utilities index. The EuroQOL-5 dimension (EQ-5D) scale is the most frequently used HRQOL instrument to calculate QALY.[26,27] In Korea, there has been only one study using EQ-5D to evaluate QOL of OVCF patients.[28] The authors evaluated QOL in postmenopausal women and reported that the QOL of OVCF patients was significantly worse than that of the control group. However, authors did not use EQ-5D index, which converts the score of EQ-5D scale into a single score. They also did not evaluate factors affecting QOL other than treatment method.
There is little research about QOL of patients with healed OVCF. The purpose of our study is to analyze QOL of patients with healed OVCF using EQ-5D. We also evaluated factors affecting QOL in OVCF patients.
MATERIALS AND METHODS
1. Study design and participants
Following institutional ethics board approval and patient agreement with informed consent, the study was performed using a questionnaire survey. The study involved an ambispective (both prospective patient recruitment and retrospective collection of information about OVCF) analysis with cross-sectional outcome assessment. From April 2015 to March 2016, total of 196 patients who had been diagnosed with vertebral compression fracture at least 6 months earlier in 2014 in the orthopedic surgery outpatient department of one of six centers were recruited. Six months is considered sufficient time for a fracture to heal. The previous diagnosis was confirmed by vertebral compression, loss of transverse trabeculae on a simple radiogram lateral view, or identification of low signal intensity in T1 and high signal intensity in T2 on magnetic resonance images. Inclusion criteria were patients over 50 years old who could understand and complete the questionnaire and consent form. Exclusion criteria were as follows: 1) patients who had secondary vertebral fracture due to infection or neoplasm; 2) patients who had severe trauma (suggesting less influence of osteoporosis); 3) patients who had neurological deficit related to OVCF; 4) patients who had other conditions significantly affecting QOL, such as metastatic malignancy or severe cardiopulmonary disease; 5) patients who had received joint replacement arthroplasty in the lower extremities prior to OVCF; 6) patients with gait disturbance for any reason prior to OVCF; 7) patients with dementia; and 8) patients on anticoagulant treatment.
2. Outcome measures
At the time of the latest visit to outpatient department, patients and orthopedic surgeons filled out OVCF questionnaires via direct interview. Surgeon's questionnaires consisted of the following: 1) patient information including age, gender, and body mass index (BMI=weight [kg]/height2 [m]; underweight <18.5, normal ≥18.5 to <23, overweight ≥23 to <25, and obese >25; according to World Health Organization [WHO] appropriate BMI for Asian population); 2) number of vertebral fracture levels; 3) interval between diagnosis and interview; 4) management method (conservative treatment or invasive treatment, such as balloon kyphoplasty, vertebroplasty, or fusion); 5) lowest bone mineral density (BMD) values (based on dual energy X-ray absorptiometry [DXA] in proximal femur and lumbar spine, divided into subgroups of T-score >−2.5 and ≤−2.5; according to WHO criteria); and 6) history of anti-osteoporotic medication use. Patient questionnaires consisted of 1) presence or absence of fracture prior to OVCF including hip, vertebrae, elbow, or wrist; 2) Oswestry disability index (ODI) score; and 3) EQ-5D scale (including EQ-visual analog scale [VAS]).
3. Assessment of QOL
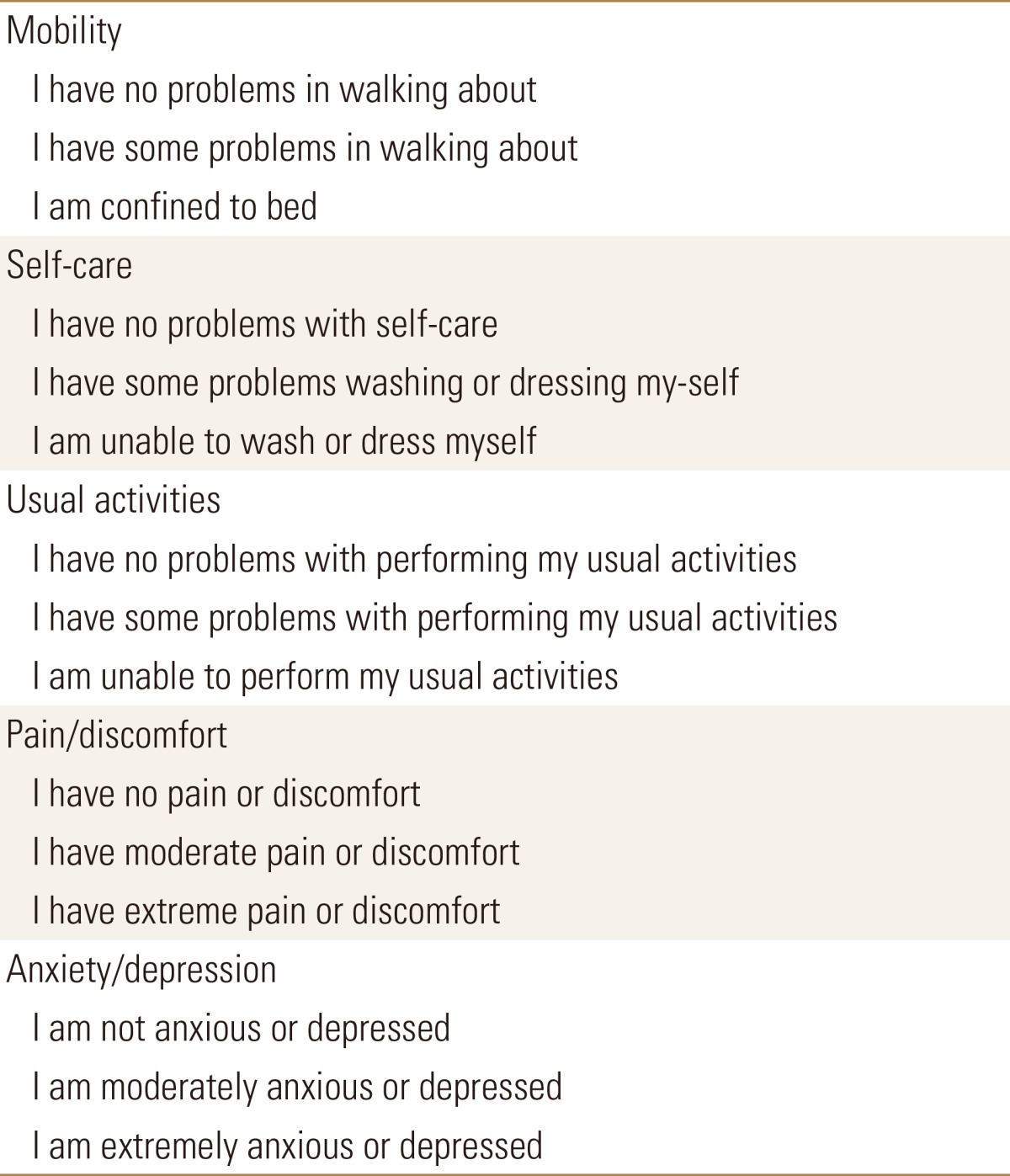
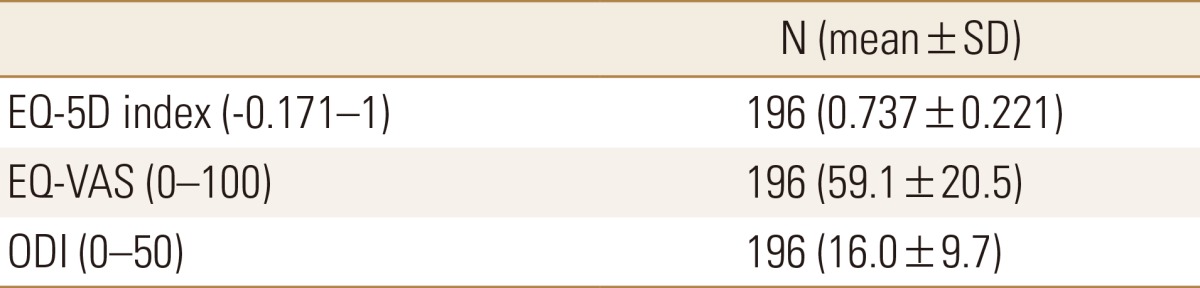
To evaluate QOL, EQ-5D scale was used. EQ-5D questionnaire is presented in Table 1. For comparison with other scales, ODI was evaluated.[29,30] EQ-5D scale has two parts, EQ-5D and EQ-VAS. Patients are asked to describe their state of health as of current day. EQ-5D provides a simple descriptive profile and a single index health status.[26] The Korean version of EQ-5D was previously validated for use in rheumatic disease.[31] Each patient's scale can be transformed into EQ-5D index using a previously reported valuation set.[25] When using this model, EQ-5D index has a range from −0.171 to 1, with 1 indicating perfect health state, 0 indicating death, and less than 0 suggesting that some health states may be worse than death. For EQ-VAS, patients responded and checked scores between 0 (worst health status) and 100 (best health status). ODI is widely used to evaluate spine-specific outcomes. ODI consisted of 10 questions, each with a score from 0 to 5, for a total maximum score of 50.
4. Statistical analysis
Means and standard deviations (SD) for the demographic data were evaluated after converting from EQ-5D scale to EQ-5D index. Means of EQ-5D index and proportion of patients with QOL problems, indicated by a response of 2 or 3, were compared with their respective normative population means [32] using a two-sided t-test. Spearman correlation coefficients were used to identify relationships between the EQ-5D index and ODI, EQ-VAS and ODI. To determine factors affecting EQ-5D index, Mann-Whitney-U-test, Spearman correlation coefficients, and one-way analysis of variance (ANOVA) were used in univariate analysis. Multiple linear regression was used for multivariable analysis. All analyses were performed using SPSS ver. 20.0 (SPSS Inc., Chicago, IL, USA). Differences were considered significant for P-values less than 0.05.
RESULTS
1. Demographic information
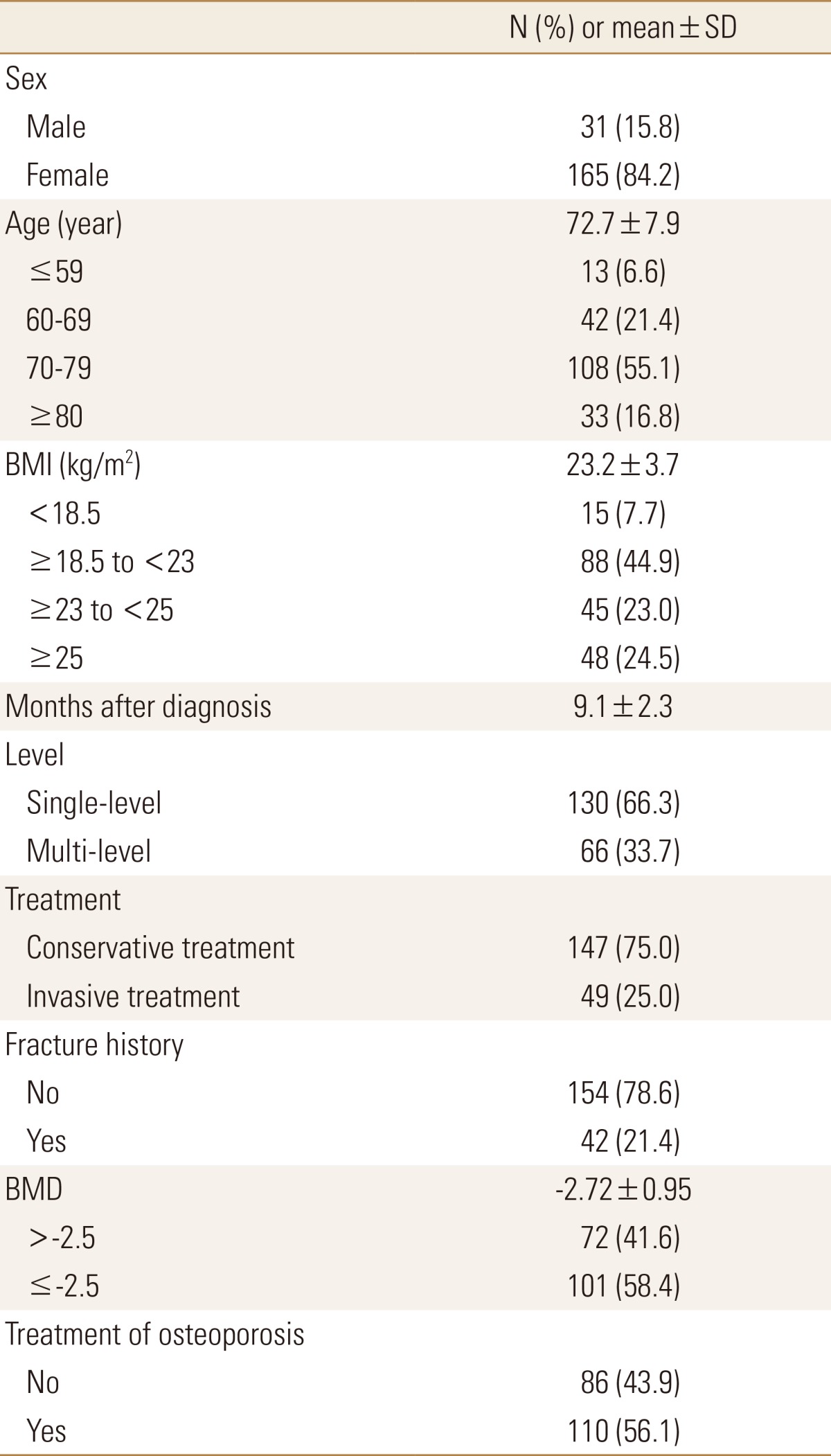
Total 196 patients with OVCF were enrolled. 31 (15.8%) were men and 165 (84.2%) were women. Average (SD) age was 72.7±7.9 years, ranging from 51 to 91 years. The mean (SD) BMI calculated based on height and weight was 23.2±3.7, ranging from 14.3 to 39.2 kg/m2. There were 15 (7.7%) underweight patients, 88 (44.9%) normal patients, 45 (23.0%) overweight patients, and 48 (24.5%) obese patients. The interval between fracture diagnosis and interview was 9.1±2.3 months, ranging from 6 to 12 months. Regarding the number of fractured vertebral levels, 130 (66.3%) patients had fracture at only one level. The rest of the population (66 [33.7%] patients) had fractures at multiple levels. For treatment, 147 (75.0%) patients underwent conservative management, and 41 (25.0%) patients underwent invasive treatment such as percutaneous balloon kyphoplasty, vertebroplasty, or vertebral fusion. Total 42 (21.4%) patients had history of fracture, with locations in the vertebrae, radius, rib, femur, and humerus. Comorbidities including hypertension, diabetes, cerebrovascular disease, coronary artery disease, severe cardiopulmonary disease, and previous arthroplasty history were present in 133 (67.9%) patients. BMD was performed using proximal femur and lumbar spine, and the lowest score was recorded. This test was performed in 173 (88.3%) patients, and their mean value (SD) was −2.72±0.95, ranging from −0.1 to −5.1. Total 101(58.4%) patients had a value less than −2.5. Total 110 (56.1%) patients were treated for osteoporosis with intravenous or oral medication. Clinical and demographic characteristics and other clinical variables are presented in Table 2.
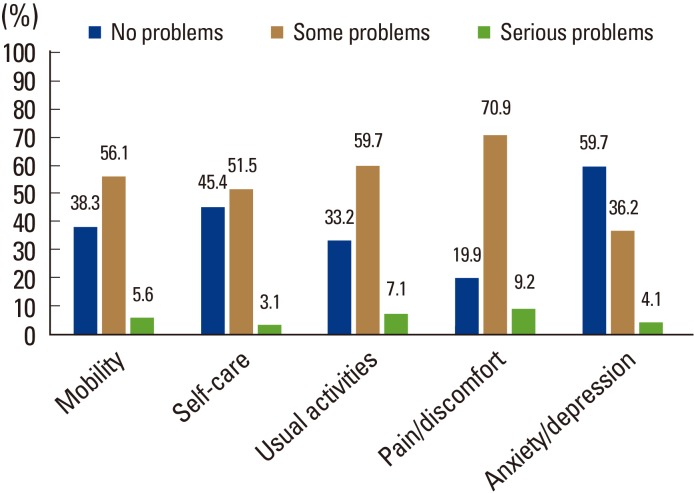
2. Assessment of QOL
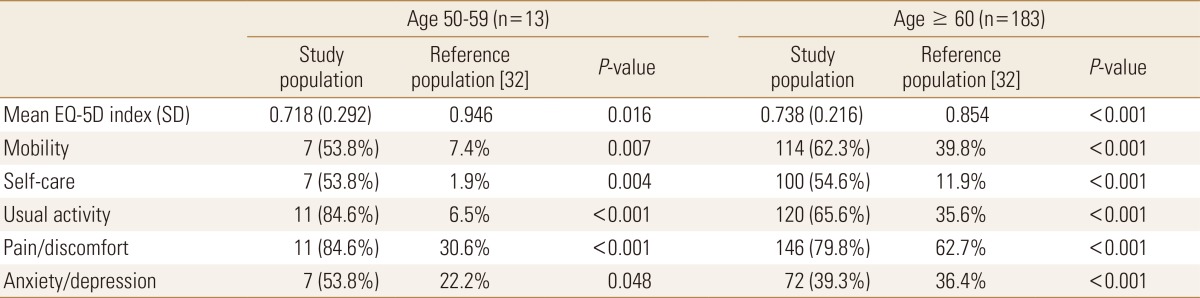
The average (SD) EQ-5D index was 0.737±0.221, ranging from −0.171 to 1.000. The median was 0.723. Total 25 (12.8%) patients had scores of 1.000, which is a perfect health state. In contrast, 4 (2.0%) patients recorded less than 0, which is a state defined as worse than death. The frequencies and percentages of participant responses to the five categorical items of EQ-5D are presented in Figure 1. In total, 61.7% of patients with OVCF had problems with mobility, 54.6% had problems with self-care, 66.7% had problems with usual activities, 80.1% had pain/discomfort, and 40.3% had anxiety/depression. The average (SD) EQ-VAS was 59.1±20.5, ranging from 0 to 100 with a median of 60.0. The mean (SD) total ODI score was 16.0±9.7, ranging from 0 to 43 (Table 3). EQ-5D index and percentage of patients with QOL problems were divided into two groups by age, 50 to 59 years old and over 60 years old, to compare with data from the normative population.[32] Table 4 shows that mean EQ-5D index was significantly lower than that of the reference population. The proportion of patients with QOL problems was also significantly higher in all dimensions of EQ-5D in both age groups compared with that in normative population.
4. Factors affecting QOL
1) Univariate analysis
BMD score was categorized by a cutoff level of −2.5. All clinical variables were analyzed with EQ-5D index (Table 6). In univariate analysis, age (Spearman's rho=−0.2, P=0.005), treatment method (P=0.005), and history of fracture (P=0.005) were significantly associated with EQ-5D index. When age was categorized by decade, patients in their ninth decade showed a significantly lower EQ-5D index than patients in their seventh and eighth decades (P=0.002, 0.022).
2) Multivariate analysis
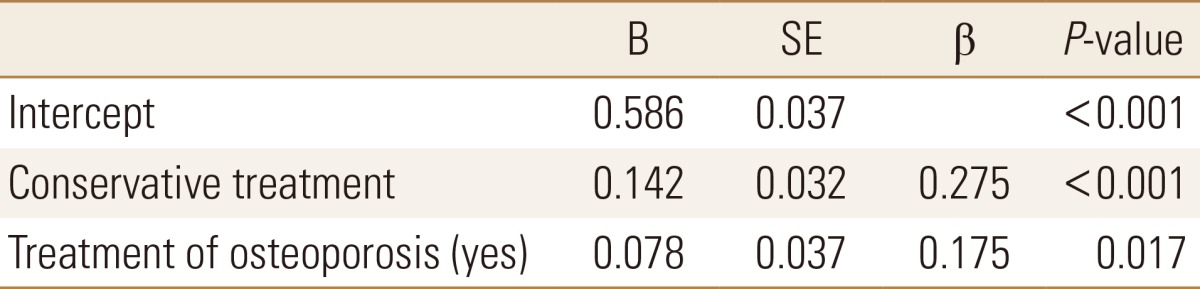
Multiple regression analysis was used to test the influence of various factors on EQ-5D index. Clinical features, gender, age, BMI, single- or multi-level fracture, conservative treatment, history of fracture, BMD, and osteoporosis treatment were included in this analysis. Among these factors, only conservative treatment (P<0.001) and utilization of osteoporotic treatment (P=0.017) significantly affected QOL (Table 7). Patient with conservative treatment (B=0.142, P<0.001) and treatment of osteoporosis (B=0.078, P=0.017) had the higher EQ-5D index than those without.
DISCUSSION
In this study, patients with healed OVCF had significantly lower HRQOL as determined by EQ-5D index than normal population. Although they had healed fractures, they had a higher frequency of problems in all dimensions, including pain/discomfort and anxiety/depression. Our results confirm prior studies that OVCF significantly lowers QOL.[4,6,9,10,11,12,13,14,23,33] Suzuki et al.[23] reported similar findings that OVCF was the starting point of long-lasting pain and disability, resulting in reduced QOL. Al-Sari et al.[24] suggested that physical limitation with spinal deformity is related to reduced QOL, but there is no clear study of long-standing QOL in OVCF to evaluate factors affecting QOL. Recovery from QOL is essential for OVCF treatment goals even after fracture healing, and it is necessary to analyze QOL and examine factors affecting QOL.
Upon investigating each dimension of EQ-5D, patients with some or severe problems (level 2 or 3) were most common in the pain/discomfort dimension. When compared with the normative population, there was a significantly higher proportion of patients in the anxiety/depression dimension. Some authors reported that it takes 2 to 4 years to achieve a pain-free state after vertebral fracture.[34,35] Our study did not estimate the time required to recover from pain, but revealed that severe pain was maintained for up to 12 months after fracture healing.
EQ-5D scale is the most frequently used HRQOL instrument to calculate QALY.[26,27] SF-36 is also widely used to evaluate HRQOL, but QALY is not reflected by SF-36.[36] In this study, the mean EQ-5D index of patients with healed OVCF was 0.737. Compared to other studies regarding QOL of various diseases, patients with OVCF had severe QOL problems. Choi et al.[37] reported that, in 1,240 patients with diabetes mellitus, the average EQ-5D index was 0.87. Kim et al.[38] reported that 200 patients with chronic obstructive pulmonary disease had an average EQ-5D index ranging from 0.61 to 0.88. Kim et al.[26] also reported that EQ-5D index of 133 patients with colorectal cancer was 0.87. These studies used the same valuation set. These findings indicate that OVCF can lead to poor QOL and cannot be ignored.
Gold [39] reported that OVCF can produce psychological impairment. Patients with OVCF have anxiety related to social implications, stress, and depression. Patients also have diminished self-esteem based on kyphosis or height loss, abdominal protrusion, and limitation of activities.[39] These findings imply that pain, discomfort of daily living, and social isolation influence the psychological state. We should carefully consider and approach these issues in patients.
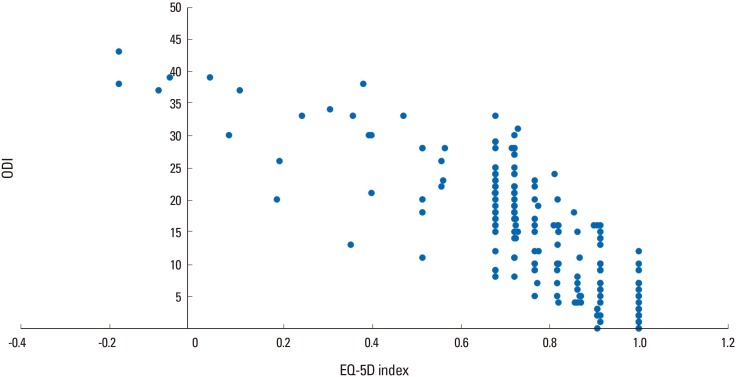
According to previous studies, EQ-5D scale is significantly correlated with ODI for evaluating back pain.[29,30] Our study also revealed a strong correlation between these variables. ODI score is widely used to measure back-specific function.[36] The Korean version of ODI score is well validated in cases of spinal disorders.[40] However, its questions outnumber those of EQ-5D, are more complicated, and include sexual activity, which is difficult to apply to elderly patients. The strong correlation of EQ-5D scale and ODI score indicates validity for evaluating QOL in OVCF with EQ-5D. Further study is necessary.
The factors affecting QOL in the present univariate analysis were age, treatment method, and history of fracture. Treatment of osteoporosis had borderline significance. According to other studies, location of compression fracture (for example, thoracic or lumbar vertebrae) can affect QOL.[33,41] But in our study, when divided into subgroups of cervical spine, thoracic spine (T1-11), thoracolumbar spine (T12-L1), and lumbar spine (L2-5), there were no significant differences in EQ-5D index.
There are controversies about the effects of invasive procedures on QOL. Some reports mentioned that percutaneous balloon kyphoplasty or vertebroplasty can improve pain and QOL.[42,43] Two randomized controlled studies have suggested that vertebroplasty and kyphoplasty are effective in pain relief.[44,45] A systematic review also mentioned that vertebroplasty or kyphoplasty can produce greater pain relief in OVCF than conservative management.[46] In contrast, two randomized clinical trials suggested that vertebroplasty was related to no significant difference in pain relief or QOL improvement compared with the control group.[42,43] Lee et al.[4] suggested that balloon kyphoplasty showed better outcomes for OVCF patients only in the first month. Also, patients in that study who received conservative treatment had significantly higher EQ-5D index. This finding is consistent with recent studies, but further trials should be undertaken to evaluate the superiority of conservative treatment in QOL of OVCF patients. Suzuki et al.[14] reported that patients with a history of previous fracture had poor QOL due to lower activity function and QOL at the time of the newly occurred fracture, and because they also had fear and anxiety of fracture.
Multivariate analysis showed that conservative treatment and osteoporosis treatment are significantly associated with QOL, despite low QOL (adjusted R2=0.104). Patients with recent osteoporotic fractures are at particularly high risk for additional fractures. Therefore, treatment of osteoporosis is generally recommended in patients with a history of spine or hip fracture, low T-score of BMD, or a fracture risk assessment tool (FRAX) score.[47] Several randomized controlled trials reported that various bisphosphonates, including alendronate, risedronate, and ibandronate, prevent osteoporotic fracture.[48,49,50,51,52] There is a report that treatment of osteoporosis is followed by increased BMD and is related to better QOL.[53] Only 56.1% of total OVCF patients in our study underwent anti-osteoporosis treatment. As mentioned above, we cannot sufficiently explain the effect on QOL, and further study including analysis of the time needed to significantly improve QOL after OVCF is needed. Further evaluation according to medication type is also warranted.
This study has several limitations. First, it was not entirely prospective. Also, patients were not randomized to treatment modality. This study was based on questionnaires, so radiologic severity of fracture was not evaluated. Lastly, it was not a longitudinal study, so follow up data were not evaluated. Therefore, we could not evaluate QOL progression or occurrence of re-fracture. However, OVCF is considered to have a relatively benign progression. When this study was designed, patients with severe bursting fracture or with neurologic deficits were excluded; therefore, some fracture patterns may not have been represented.
However, this study has powerful strengths. First, this trial assessed a reasonably large number of patients with healed fracture from multiple centers. Patients had homogeneous diagnoses because they were diagnosed with OVCF during similar periods and were recruited in specific period. The correlation between QOL and osteoporosis was evaluated based on BMD and osteoporosis treatment.
CONCLUSION
OVCF showed markedly low QOL in several dimensions, including psychological impairment, even after fracture healing. Treatment of osteoporosis and OVCF are factors that affect QOL and should be considered carefully during management. When treating patients with OVCF, a multidisciplinary approach is essential to improve QOL.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






